Zhu Jinfeng, Zeng Wei, Ge Lei, Yang Xinhui, Wang Qisan, Wang Haijiang
Department of Gastrointestinal Surgery, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang.
Department of Hematology and Oncology, Shenzhen University General Hospital, Shenzhen, Guangdong.
Medicine (Baltimore). 2019 Apr;98(17):e15241. doi: 10.1097/MD.0000000000015241.
The differences in efficacy between capecitabine and 5-fuorouracil (5-FU) in neoadjuvant chemoradiotherapy (CRT) of locally advanced rectal cancer (LARC) are not well recognized. We performed this meta-analysis to analyze the effect of capecitabine and 5-FU on neoadjuvant CRT to more accurately understand the differences between the 2 drugs.
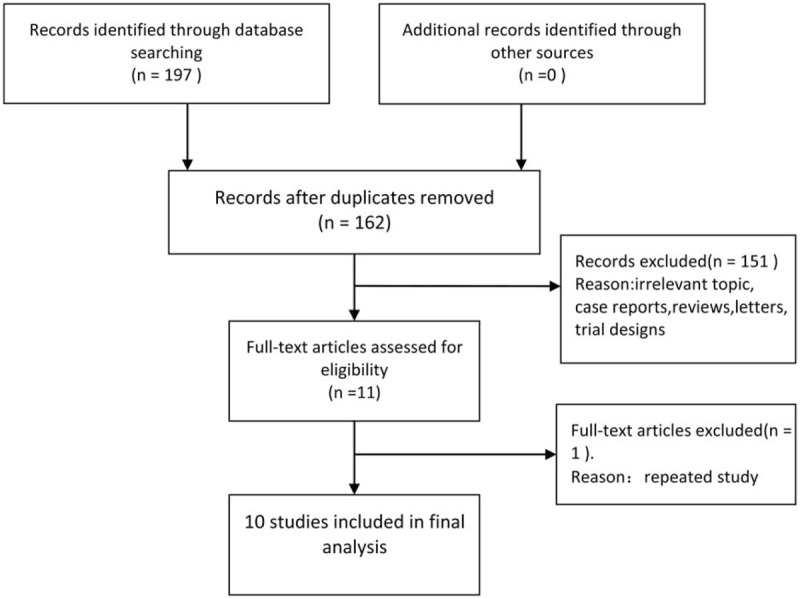
MEDLINE, EMBASE, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Database were performed to identify all published studies investigating the efficacy of capecitabine in neoadjuvant CRT of LARC versus 5-FU before August, 2017. Primary endpoint was the odds ratio (OR) for improving pathological complete response (pCR) rate of patients with LARC. Secondary endpoints were the ORs of efficiency for downstaging tumor and increasing R0 resection in patients with LARC. Safety analyses were also performed. The OR was the principal measurement of effect, which was calculated as capecitabine group versus 5-FU group, and was presented as a point estimate with 95% confidence intervals (CIs). All calculations and statistical tests were performed using RevMan 5.3 software.
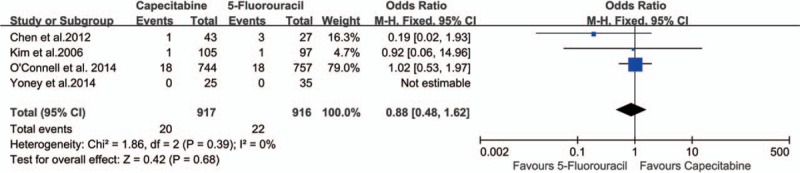
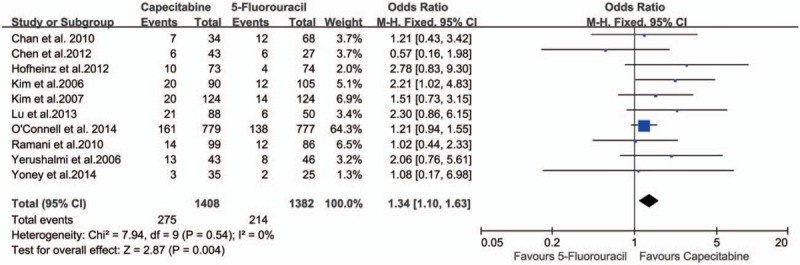
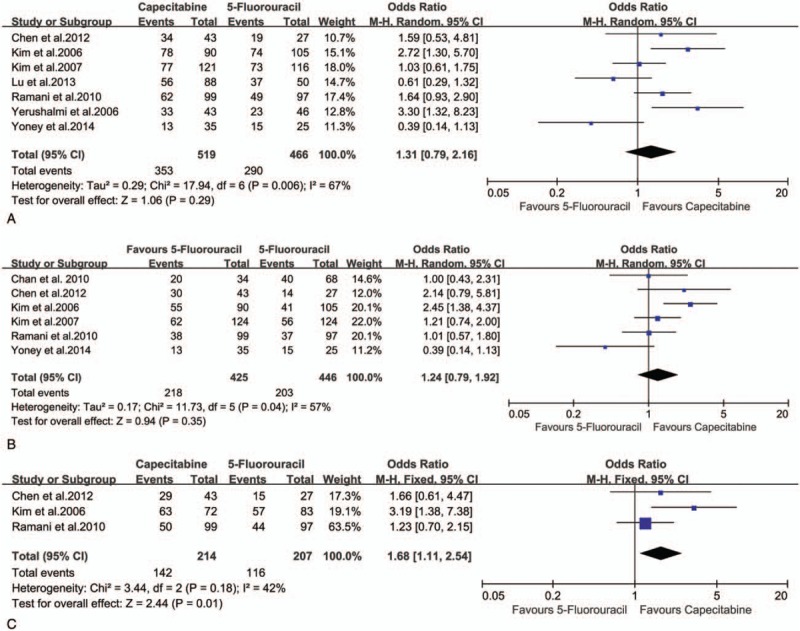
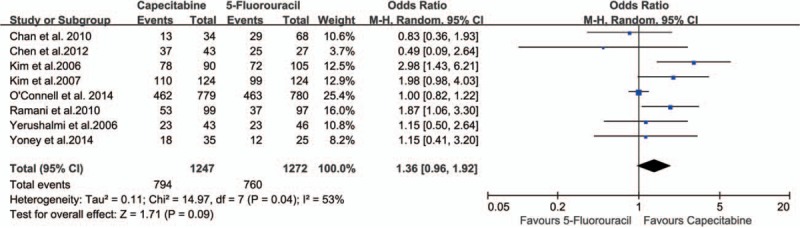
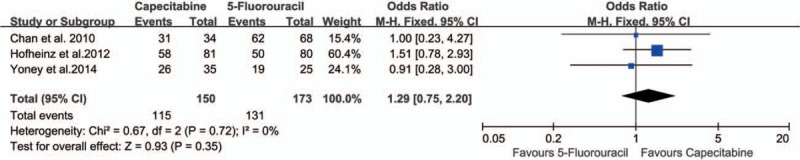
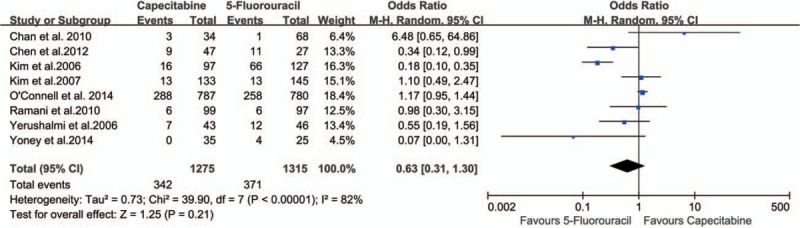
In all, 2916 patients with LARC enrolled in the 10 studies were divided into capecitabine group (n = 1451) and 5-FU group (n = 1465). The meta-analysis showed that capecitabine improved pCR (OR 1.34, 95% CI 1.10-1.63), and R0 resection rate (OR 1.92, 95% CI 1.10-3.36). There were no statistically significant differences either in overall downstaging rate (OR 1.31, 95% CI 0.79-2.16) or in the tumor downstaging rate (OR 1.24, 95% CI 0.79-1.92), but there was a significant difference of the nodal downstaging rate between the 2 groups (OR 1.68, 95% CI 1.11-2.54). There was no statistically significant difference in sphincter preservation rate between the 2 groups (OR 1.36, 95% CI 0.96-1.92). No obvious safety concerns about mortality and complications were raised in these studies. There were no statistically significant differences in 3-year disease-free-survival (OR 1.29, 95% CI 0.75-2.20), and in grade 3 to 4 acute toxicity during CRT (OR 0.63, 95% CI 0.31-1.30).
Compared with 5-FU-based neoadjuvant CRT, capecitabine-based neoadjuvant CRT can safely improve pCR, nodal down-staging, ad R0 resection of patients with LARC.
在局部晚期直肠癌(LARC)的新辅助放化疗(CRT)中,卡培他滨与5-氟尿嘧啶(5-FU)疗效的差异尚未得到充分认识。我们进行了这项荟萃分析,以分析卡培他滨和5-FU对新辅助CRT的影响,从而更准确地了解这两种药物之间的差异。
检索MEDLINE、EMBASE、Cochrane图书馆、中国知网和万方数据库,以识别2017年8月之前发表的所有研究卡培他滨与5-FU在LARC新辅助CRT中疗效的研究。主要终点是LARC患者病理完全缓解(pCR)率提高的比值比(OR)。次要终点是LARC患者肿瘤降期和R0切除效率的OR。还进行了安全性分析。OR是主要的效应测量指标,计算为卡培他滨组与5-FU组之比,并以95%置信区间(CI)的点估计值表示。所有计算和统计检验均使用RevMan 5.3软件进行。
10项研究共纳入2916例LARC患者,分为卡培他滨组(n = 1451)和5-FU组(n = 1465)。荟萃分析表明,卡培他滨提高了pCR(OR 1.34,95%CI 1.10 - 1.63)和R0切除率(OR 1.92,95%CI 1.10 - 3.36)。总体降期率(OR 1.31,95%CI 0.79 - 2.16)和肿瘤降期率(OR 1.24,95%CI 0.79 - 1.92)在两组间无统计学显著差异,但两组间淋巴结降期率有显著差异(OR 1.68,95%CI 1.11 - 2.54)。两组间括约肌保留率无统计学显著差异(OR 1.36,95%CI 0.96 - 1.92)。这些研究中未提出关于死亡率和并发症的明显安全问题。3年无病生存率(OR 1.29,95%CI 0.75 - 2.20)和CRT期间3 - 4级急性毒性(OR 0.63,95%CI 0.31 - 1.30)在两组间无统计学显著差异。
与基于5-FU的新辅助CRT相比,基于卡培他滨的新辅助CRT可安全地提高LARC患者的pCR、淋巴结降期和R0切除率。