Division of Cardiology, Department of Internal Medicine and Radiology, University of Alabama at Birmingham, Birmingham, Alabama, United States of America.
Brigham and Women's Hospital Heart and Vascular Center and Harvard Medical School, Boston, Massachusetts, United States of America.
PLoS Med. 2019 Apr 29;16(4):e1002797. doi: 10.1371/journal.pmed.1002797. eCollection 2019 Apr.
The efficacy, safety, and clinical importance of extended-duration thromboprophylaxis (EDT) for prevention of venous thromboembolism (VTE) in medical patients remain unclear. We compared the efficacy and safety of EDT in patients hospitalized for medical illness.
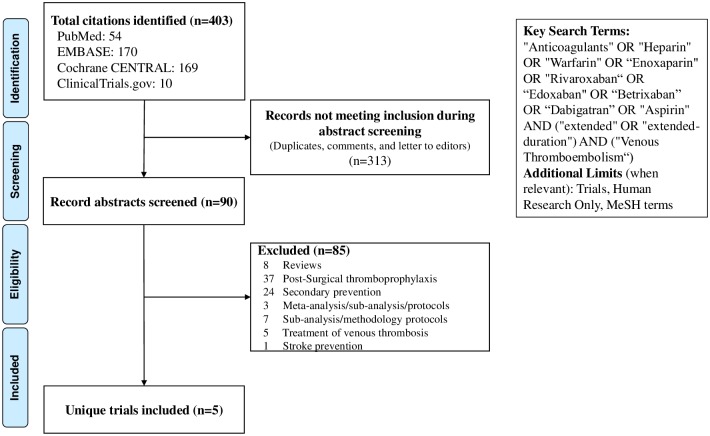
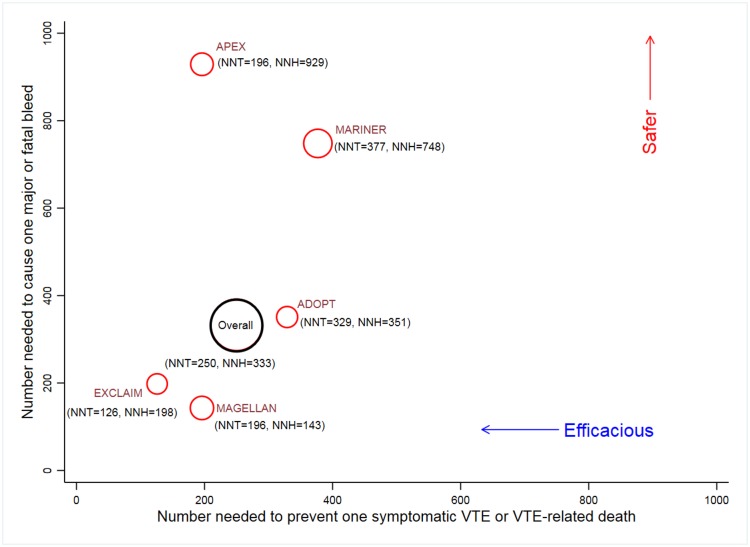
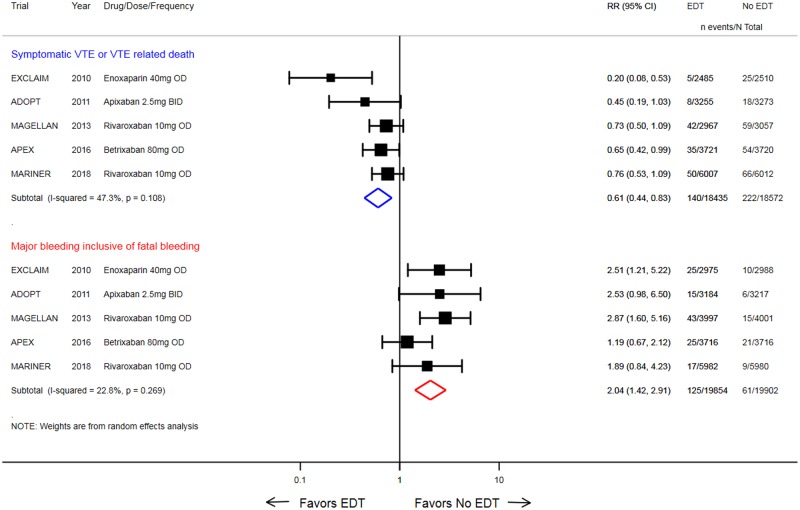
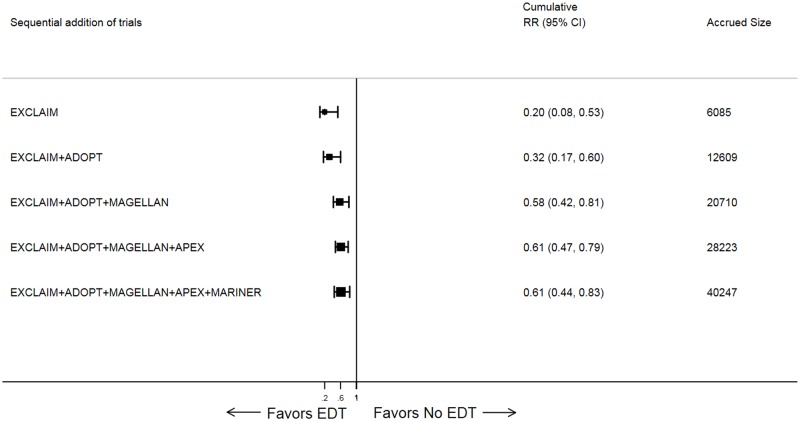
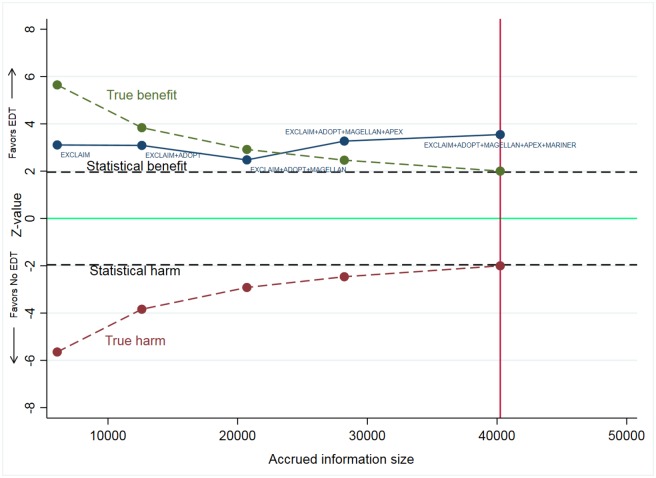
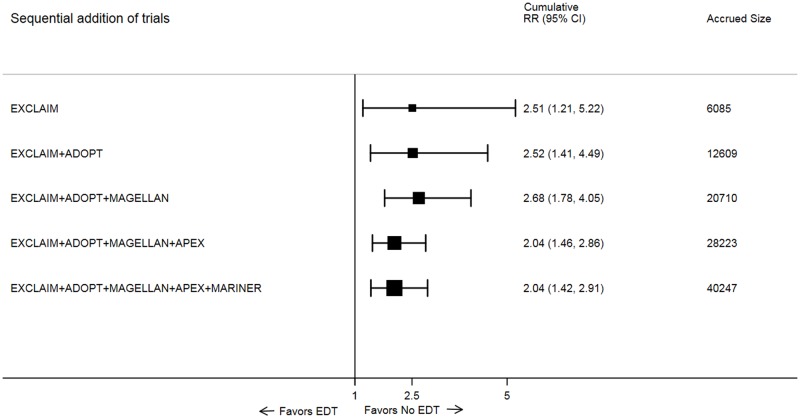
Electronic databases of PubMed/MEDLINE, EMBASE, Cochrane Central, and ClinicalTrials.gov were searched from inception to March 21, 2019. We included randomized clinical trials (RCTs) reporting use of EDT for prevention of VTE. We performed trial sequential and cumulative meta-analyses to evaluate EDT effects on the primary efficacy endpoint of symptomatic VTE or VTE-related death, International Society on Thrombosis and Haemostasis (ISTH) major or fatal bleeding, and all-cause mortality. The pooled number needed to treat (NNT) to prevent one symptomatic or fatal VTE event and the number needed to harm (NNH) to cause one major or fatal bleeding event were calculated. Across 5 RCTs with 40,247 patients (mean age: 67-77 years, proportion of women: 48%-54%, most common reason for admission: heart failure), the duration of EDT ranged from 24-47 days. EDT reduced symptomatic VTE or VTE-related death compared with standard of care (0.8% versus 1.2%; risk ratio [RR]: 0.61, 95% confidence interval [CI]: 0.44-0.83; p = 0.002). EDT increased risk of ISTH major or fatal bleeding (0.6% versus 0.3%; RR: 2.04, 95% CI: 1.42-2.91; p < 0.001) in both meta-analyses and trial sequential analyses. Pooled NNT to prevent one symptomatic VTE or VTE-related death was 250 (95% CI: 167-500), whereas NNH to cause one major or fatal bleeding event was 333 (95% CI: 200-1,000). Limitations of the study include variation in enrollment criteria, individual therapies, duration of EDT, and VTE detection protocols across included trials.
In this systematic review and meta-analysis of 5 randomized trials, we observed that use of a post-hospital discharge EDT strategy for a 4-to-6-week period reduced symptomatic or fatal VTE events at the expense of increased risk of major or fatal bleeding. Further investigations are still required to define the risks and benefits in discrete medically ill cohorts, evaluate cost-effectiveness, and develop pathways for targeted implementation of this postdischarge EDT strategy.
PROSPERO CRD42018109151.
延长疗程的血栓预防(EDT)在预防医学患者静脉血栓栓塞症(VTE)方面的疗效、安全性和临床重要性仍不清楚。我们比较了住院治疗的医学疾病患者中 ED 的疗效和安全性。
从建立到 2019 年 3 月 21 日,我们在 PubMed/MEDLINE、EMBASE、Cochrane 中央和 ClinicalTrials.gov 的电子数据库中进行了搜索。我们纳入了报告使用 EDT 预防 VTE 的随机临床试验(RCT)。我们进行了试验序贯和累积荟萃分析,以评估 ED 在主要疗效终点(有症状 VTE 或 VTE 相关死亡、国际血栓与止血学会(ISTH)主要或致命性出血)和全因死亡率方面的效果。计算了预防一个有症状或致命性 VTE 事件和导致一个主要或致命性出血事件所需的治疗人数(NNT)和所需的危害人数(NNH)。在 5 项涉及 40247 名患者(平均年龄:67-77 岁,女性比例:48%-54%,最常见的入院原因:心力衰竭)的 RCT 中,EDT 的持续时间为 24-47 天。与标准治疗相比,EDT 降低了有症状 VTE 或 VTE 相关死亡的风险(0.8% 与 1.2%;风险比 [RR]:0.61,95%置信区间 [CI]:0.44-0.83;p = 0.002)。EDT 增加了 ISTH 主要或致命性出血的风险(0.6% 与 0.3%;RR:2.04,95%CI:1.42-2.91;p < 0.001),这在两项荟萃分析和试验序贯分析中都是如此。预防一个有症状 VTE 或 VTE 相关死亡的 NNT 为 250(95%CI:167-500),而导致一个主要或致命性出血事件的 NNH 为 333(95%CI:200-1,000)。该研究的局限性包括纳入标准、个体治疗、EDT 持续时间和纳入试验中的 VTE 检测方案的变化。
在这项对 5 项随机试验的系统评价和荟萃分析中,我们观察到,在住院期间和出院后使用长达 4-6 周的 EDT 策略可降低有症状或致命性 VTE 事件的发生,但会增加主要或致命性出血的风险。仍需要进一步研究以确定在特定的医学疾病患者亚群中,这种 EDT 策略的风险和获益,评估成本效益,并制定针对该策略的实施途径。
PROSPERO CRD42018109151。