Spyropoulos Alex C, Goldin Mark, Koulas Ioannis, Solomon Jeffrey, Qiu Michael, Ngu Sam, Smith Kolton, Leung Tungming, Ochani Kanta, Malik Fatima, Cohen Stuart L, Giannis Dimitrios, Khan Sundas, McGinn Thomas
Institute of Health System Science, Feinstein Institutes for Medical Research, Northwell Health, Manhasset, New York, USA.
Department of Medicine, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, New York, USA.
JACC Adv. 2023 Sep 13;2(8):100597. doi: 10.1016/j.jacadv.2023.100597. eCollection 2023 Oct.
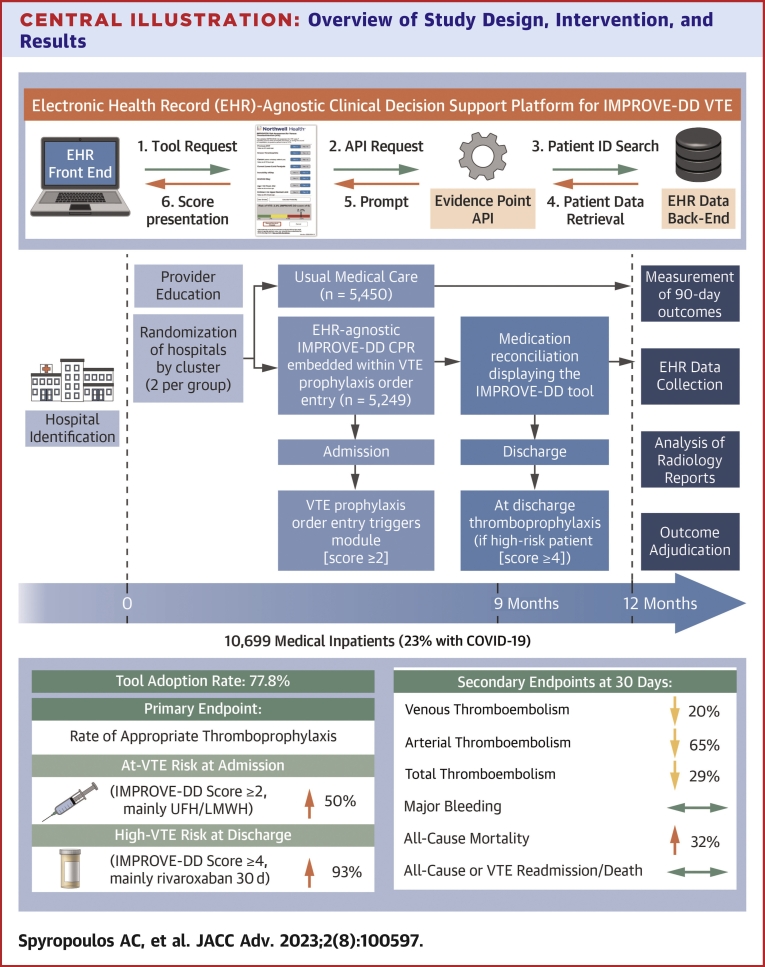
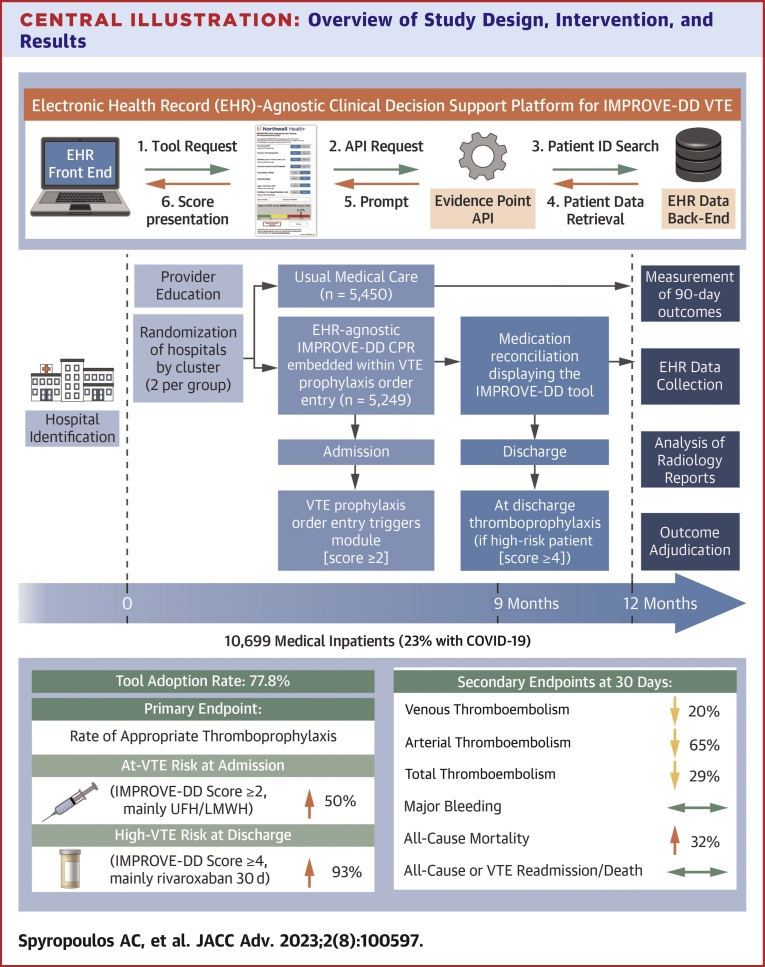
Thromboprophylaxis for medically ill patients during hospitalization and postdischarge remains underutilized. Clinical decision support (CDS) may address this need if embedded within workflow, interchangeable among electronic health records (EHRs), and anchored on a validated model.
The purpose of this study was to assess the clinical impact of a universal EHR-integrated CDS tool based on the International Medical Prevention Registry on Venous Thromboembolism plus D-Dimer venous thromboembolism model.
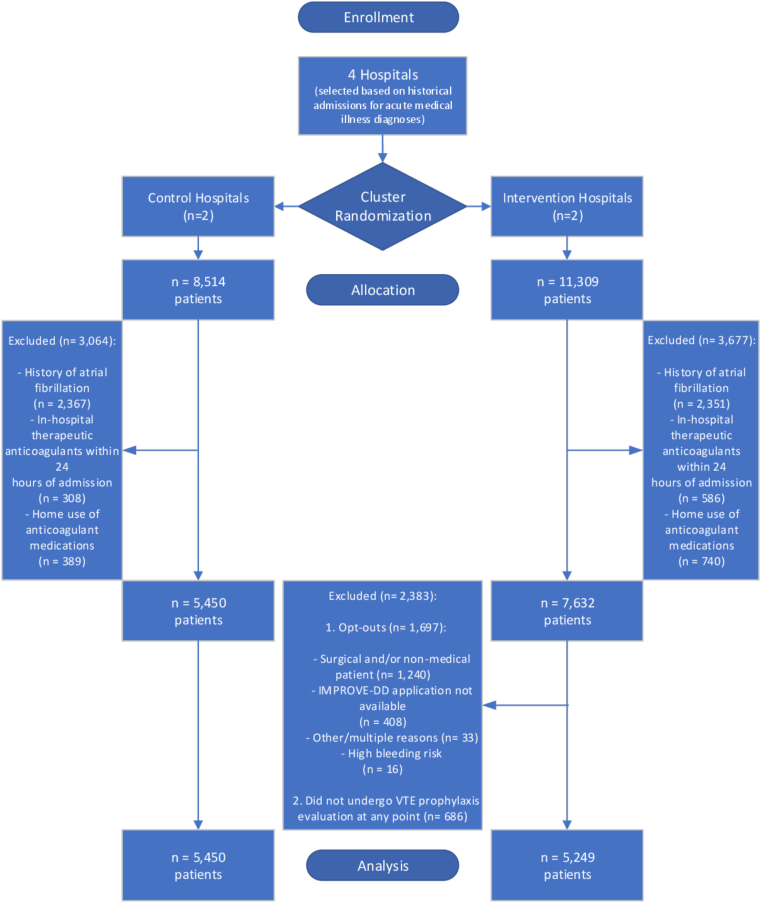
This was a cluster randomized trial of 4 tertiary academic hospitals from December 21, 2020 to January 21, 2022. Inpatients over age 60 with key medical illnesses were eligible. We embedded CDS at admission and discharge. Hospitals were randomized to intervention (CDS; n = 2) vs usual care (n = 2) groups. The primary outcome was rate of appropriate thromboprophylaxis. Secondary outcomes included venous, arterial, and total thromboembolism, major bleeding, and all-cause mortality through 30 days postdischarge.
After exclusions, 10,699 of 19,823 patients were analyzed. Intervention group tool adoption was 77.8%. Appropriate thromboprophylaxis was increased at intervention hospitals, both inpatient (80.1% vs 72.5%, OR: 1.52, 95% CI: 1.39-1.67) and at discharge (13.6% vs 7.5%, OR: 1.93, 95% CI: 1.60-2.33). There were fewer venous (2.7% vs 3.3%, OR: 0.80, 95% CI: 0.64-1.00), arterial (0.25% vs 0.70%, OR: 0.35, 95% CI: 0.19-0.67), and total thromboembolisms (2.9% vs 4.0%, OR: 0.71, 95% CI: 0.58-0.88) at intervention hospitals. Major bleeding was rare and did not differ between groups. Mortality was higher at intervention hospitals (9.1% vs 7.0%, OR: 1.32, 95% CI: 1.15-1.53).
EHR-embedded CDS increased appropriate thromboprophylaxis and reduced thromboembolism without increasing major bleeding in medically ill inpatients. Mortality was higher at intervention hospitals.
对于内科疾病患者,住院期间及出院后的血栓预防措施仍未得到充分利用。如果临床决策支持(CDS)能融入工作流程、在电子健康记录(EHR)之间可互换,并基于经过验证的模型,那么它可能满足这一需求。
本研究旨在评估基于国际静脉血栓栓塞症医学预防登记册加D - 二聚体静脉血栓栓塞症模型的通用电子健康记录集成临床决策支持工具的临床影响。
这是一项于2020年12月21日至2022年1月21日对4家三级学术医院进行的整群随机试验。年龄超过60岁且患有主要内科疾病的住院患者符合条件。我们在入院和出院时嵌入了临床决策支持。医院被随机分为干预组(临床决策支持;n = 2)和常规治疗组(n = 2)。主要结局是适当血栓预防的比例。次要结局包括静脉、动脉和总血栓栓塞、大出血以及出院后30天内的全因死亡率。
排除后,对19823例患者中的10699例进行了分析。干预组工具采用率为77.8%。干预医院的适当血栓预防有所增加,无论是住院期间(80.1%对72.5%,OR:1.52,95%CI:1.39 - 1.67)还是出院时(13.6%对7.5%,OR:1.93,95%CI:1.60 - 2.33)。干预医院的静脉血栓栓塞(2.7%对3.3%,OR:0.80,95%CI:0.64 - 1.00)、动脉血栓栓塞(0.25%对0.70%,OR:0.35,95%CI:0.19 - 0.67)和总血栓栓塞(2.9%对4.0%,OR:0.71,95%CI:0.58 - 0.88)较少。大出血很少见,两组之间无差异。干预医院的死亡率较高(9.1%对7.0%,OR:1.32,95%CI:1.15 - 1.53)。
电子健康记录嵌入的临床决策支持增加了适当的血栓预防并减少了血栓栓塞,而不会增加内科疾病住院患者的大出血。干预医院的死亡率较高。