Department of Pharmacy Practice, College of Pharmacy, Mercer University, Atlanta, GA, United States of America.
Influenza Division, National Center for Immunization and Respiration Diseases, (CDC), Atlanta, GA, United States of America.
PLoS One. 2019 Apr 29;14(4):e0213499. doi: 10.1371/journal.pone.0213499. eCollection 2019.
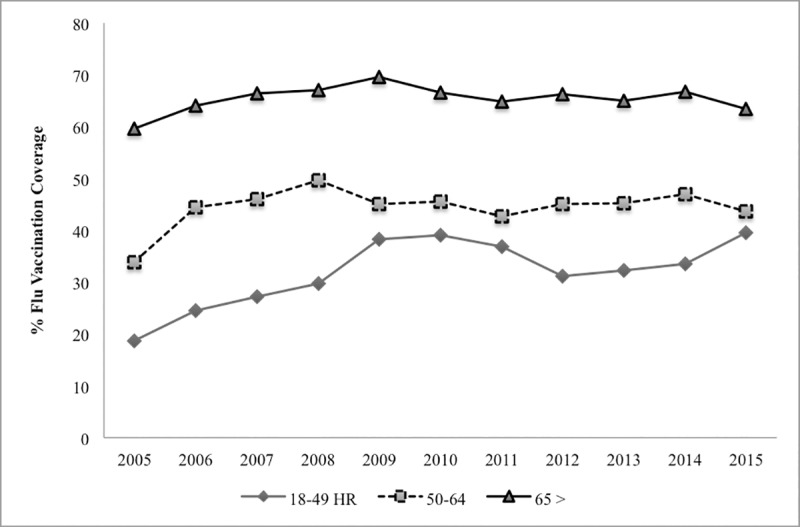
Although influenza vaccination has been shown to reduce the incidence of major adverse cardiac events (MACE) among those with existing cardiovascular disease (CVD), in the 2015-16 season, coverage for persons with heart disease was only 48% in the US.
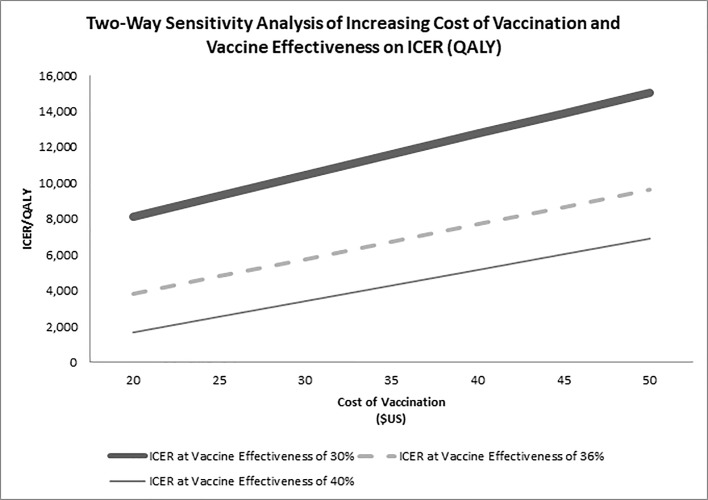
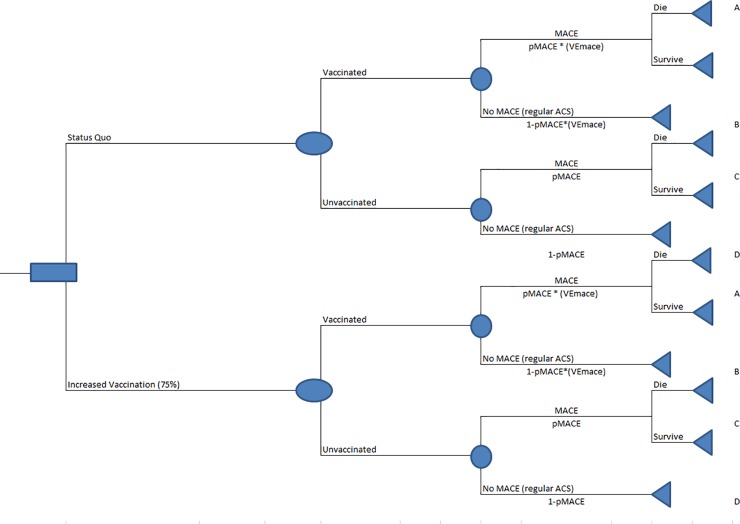
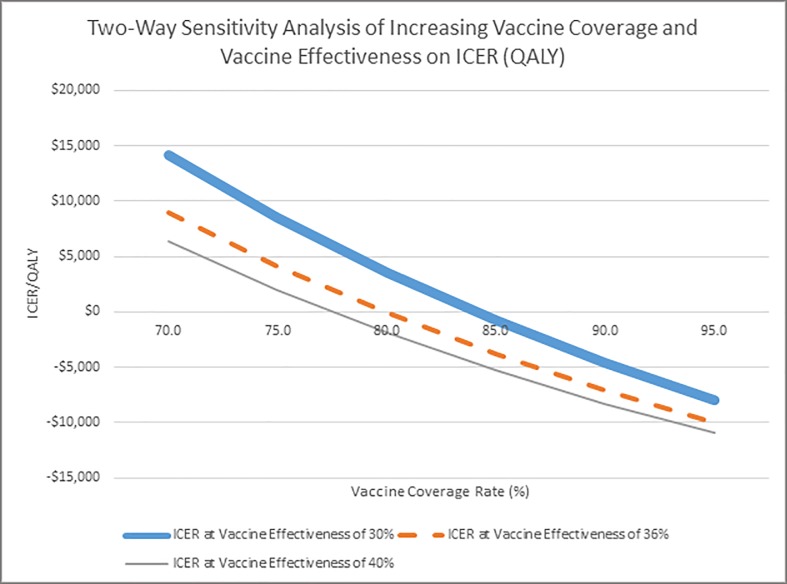
We built a Monte Carlo (probabilistic) spreadsheet-based decision tree in 2018 to estimate the cost-effectiveness of increased influenza vaccination to prevent MACE readmissions. We based our model on current US influenza vaccination coverage of the estimated 493,750 US acute coronary syndrome (ACS) patients from the healthcare payer perspective. We excluded outpatient costs and time lost from work and included only hospitalization and vaccination costs. We also estimated the incremental cost/MACE case averted and incremental cost/QALY gained (ICER) if 75% hospitalized ACS patients were vaccinated by discharge and estimated the impact of increasing vaccination coverage incrementally by 5% up to 95% in a sensitivity analysis, among hospitalized adults aged ≥ 65 years and 18-64 years, and varying vaccine effectiveness from 30-40%.
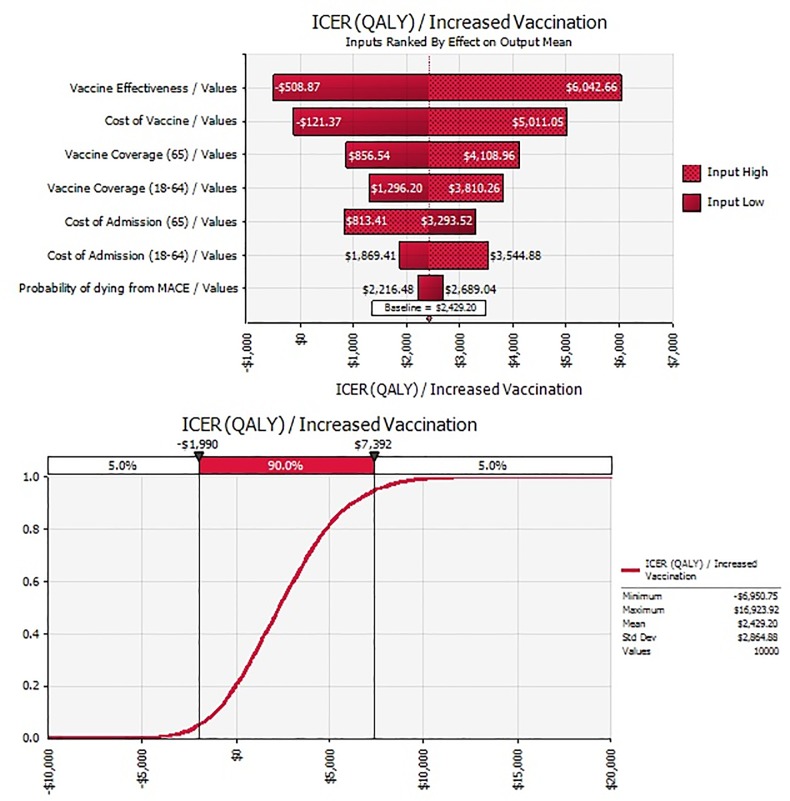
At 75% vaccination coverage by discharge, vaccination was cost-saving from the healthcare payer perspective in adults ≥ 65 years and the ICER was $12,680/QALY (95% CI: 6,273-20,264) in adults 18-64 years and $2,400 (95% CI: -1,992-7,398) in all adults 18 + years. These resulted in ~ 500 (95% CI: 439-625) additional averted MACEs/year for all adult patients aged ≥18 years and added ~700 (95% CI: 578-825) QALYs. In the sensitivity analysis, vaccination becomes cost-saving in adults 18+years after about 80% vaccination rate. To achieve 75% vaccination rate in all adults aged ≥ 18 years will require an additional cost of $3 million. The effectiveness of the vaccine, cost of vaccination, and vaccination coverage rate had the most impact on the results.
Increasing vaccination rate among hospitalized ACS patients has a favorable cost-effectiveness profile and becomes cost-saving when at least 80% are vaccinated.
尽管流感疫苗接种已被证明可以降低已有心血管疾病(CVD)患者发生主要不良心脏事件(MACE)的发生率,但在 2015-16 季节,心脏病患者的疫苗接种覆盖率仅为美国的 48%。
我们于 2018 年建立了一个基于蒙特卡罗(概率)电子表格的决策树,以估计增加流感疫苗接种以预防 MACE 再入院的成本效益。我们的模型基于当前美国流感疫苗接种覆盖率,估计有 493750 名美国急性冠脉综合征(ACS)患者从医疗支付者的角度来看。我们排除了门诊费用和因工作而损失的时间,只包括住院和疫苗接种费用。我们还估计了如果 75%的住院 ACS 患者在出院时接种疫苗,每例 MACE 预防的增量成本和每例 QALY 获得的增量成本(ICER),并在敏感性分析中按 5%的增量递增增加疫苗接种覆盖率,直至 95%,在≥65 岁和 18-64 岁的住院成年人中,以及疫苗有效性从 30%到 40%不等。
在出院时达到 75%的疫苗接种率,从医疗支付者的角度来看,疫苗接种在≥65 岁的成年人中是节省成本的,在 18-64 岁的成年人中,ICER 为 12680 美元/QALY(95%CI:6273-20264),在所有≥18 岁的成年人中为 2400 美元(95%CI:-1992-7398)。这导致所有≥18 岁的成年患者每年额外预防约 500 例(95%CI:439-625)MACE,额外增加约 700 例(95%CI:578-825)QALY。在敏感性分析中,在接种率约为 80%后,18 岁以上的成年人的疫苗接种变得节省成本。要使所有≥18 岁的成年人的疫苗接种率达到 75%,还需要额外花费 300 万美元。疫苗的有效性、疫苗接种成本和疫苗接种率对结果影响最大。
增加住院 ACS 患者的疫苗接种率具有良好的成本效益,当至少 80%的患者接种疫苗时,疫苗接种就变得节省成本。