Kim Na Young, Chun Duk-Hee, Kim So Yeon, Kim Nam Kyu, Baik Seung Hyuk, Hong Jung Hwa, Kim Kyung Sub, Shin Cheung-Soo
Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea.
Department of Anesthesiology and Pain Medicine, CHA Bundang Medical Center, CHA University school of Medicine, 59 Yatap-ro, Seongnam, Gyeonggi-do 13496, Korea.
J Clin Med. 2019 Apr 29;8(5):589. doi: 10.3390/jcm8050589.
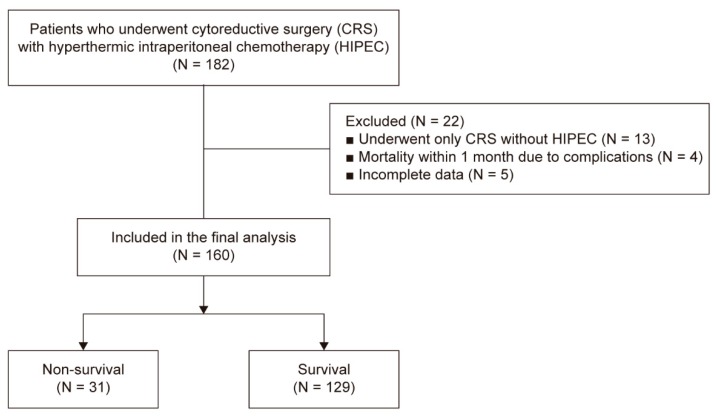
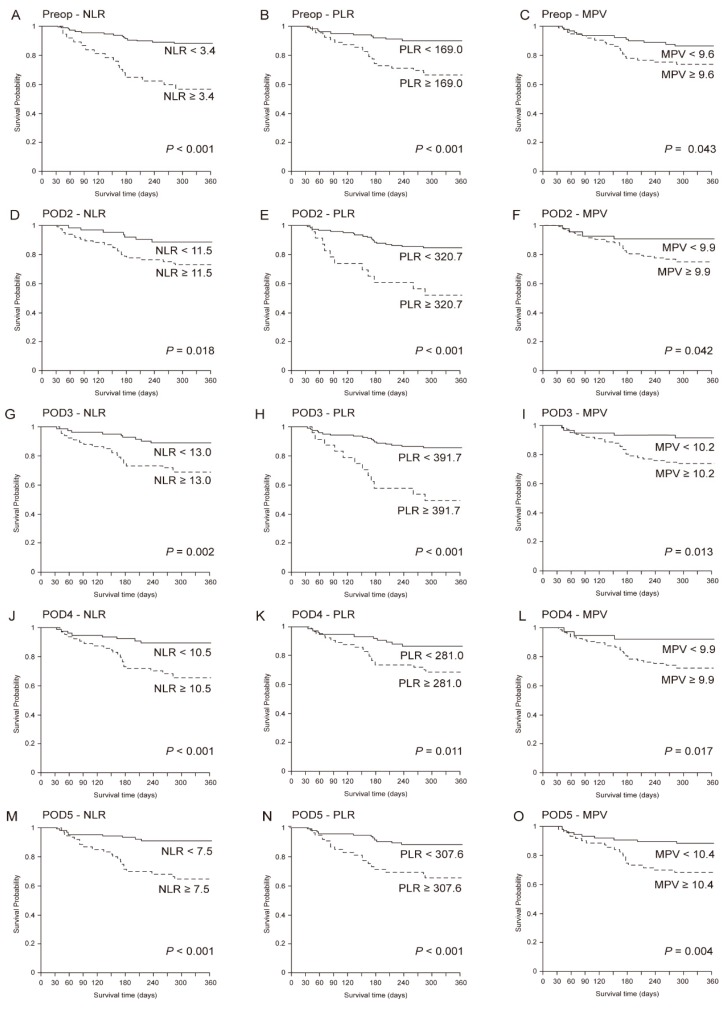
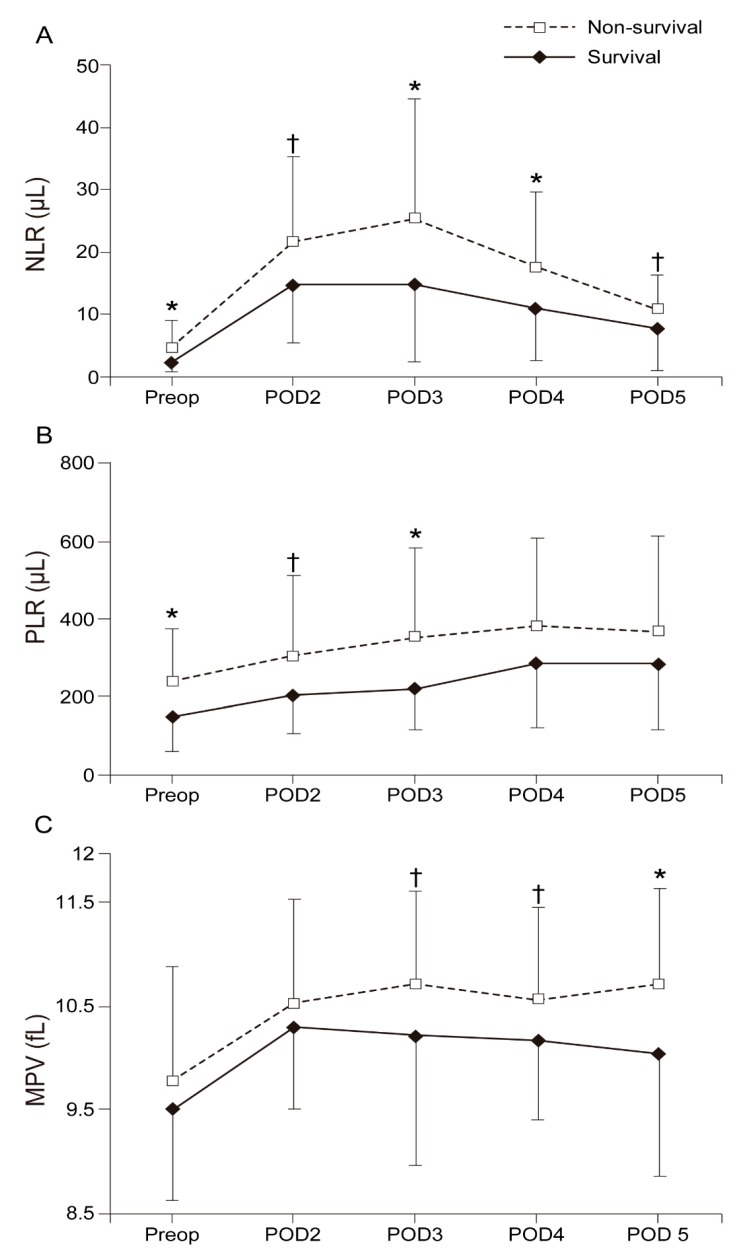
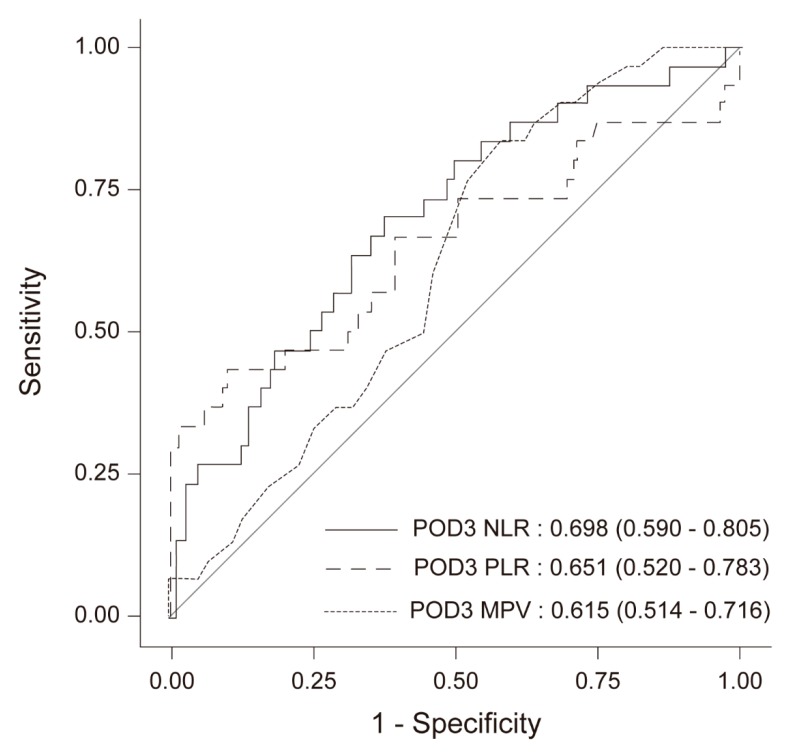
The neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and mean platelet volume (MPV) have been reported to be associated with the prognosis of various types of tumors. This study evaluated the prognostic value and clinical use of inflammatory markers for predicting 1-year survival in patients undergoing cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC). This retrospective study included 160 patients who underwent CRS with HIPEC between July 2014 and April 2017. Data on NLR, PLR, and MPV were collected preoperatively and on postoperative days (POD) 1, 2, 3, 4, and 5. In a multivariate analysis using a cox proportional hazard regression model, higher values of preoperative NLR and MPV, PLR, and MPV on POD 2, 3, and 5 were associated with reduced 1-year survival after CRS with HIPEC. Patients with increased MPV showed lower rates of 1-year survival following CRS with HIPEC. In addition, elevated preoperative NLR and postoperative PLR were correlated with poor survival. These markers are able to stratify patients by risk profile, which may ultimately improve perioperative management and be helpful in improving outcomes following CRS with HIPEC.
据报道,中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)及平均血小板体积(MPV)与多种类型肿瘤的预后相关。本研究评估了炎症标志物对接受减瘤手术(CRS)联合热灌注腹腔化疗(HIPEC)患者1年生存率预测的预后价值及临床应用。这项回顾性研究纳入了2014年7月至2017年4月期间160例行CRS联合HIPEC的患者。收集术前及术后第1、2、3、4和5天的NLR、PLR和MPV数据。在使用Cox比例风险回归模型的多因素分析中,术前较高的NLR、术前及术后第2、3和5天较高的PLR及MPV与CRS联合HIPEC术后1年生存率降低相关。MPV升高的患者CRS联合HIPEC术后1年生存率较低。此外,术前NLR升高及术后PLR升高与生存不良相关。这些标志物能够根据风险特征对患者进行分层,这最终可能改善围手术期管理,并有助于改善CRS联合HIPEC后的预后。