Directorate of Pediatrics & Child Health, Mulago National Referral Hospital, P.O. Box 23491, Kampala, Uganda.
Division of Pediatric Infectious Diseases, University of California, 550 16th St. 4th floor, San Francisco, CA, 94158, USA.
BMC Public Health. 2019 Apr 29;19(1):446. doi: 10.1186/s12889-019-6821-2.
Childhood tuberculosis (TB) diagnoses often lack microbiologic confirmation and require empiric treatment. Barriers to empiric treatment include concern for poor outcomes and adverse effects. We thus determined the outcomes of empiric TB treatment from a retrospective cohort of children at a national referral hospital in Kampala, Uganda from 2010 to 2015.
Children were diagnosed clinically and followed through treatment. Demographics, clinical data, outcome and any adverse events were extracted from patient charts. A favorable outcome was defined as a child completing treatment with clinical improvement. We performed logistic regression to assess factors associated with loss to follow up and death.
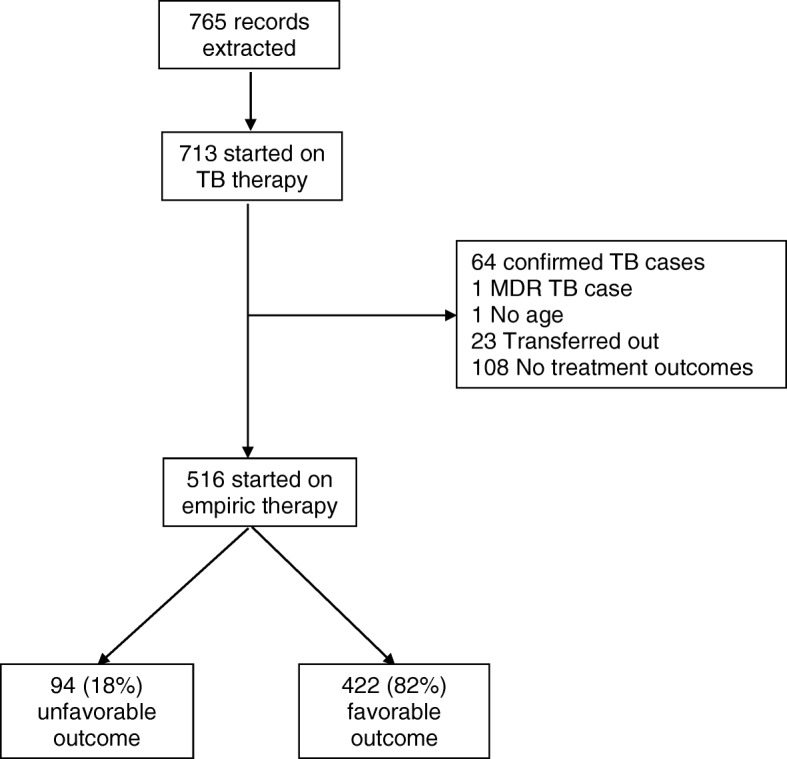
Of 516 children, median age was 36 months (IQR 15-73), 55% (95% CI 51-60%) were male, and HIV prevalence was 6% (95% CI 4-9%). The majority (n = 422, 82, 95% CI 78-85%) had a favorable outcome, with no adverse events that required treatment discontinuation. The most common unfavorable outcomes were loss to follow-up (57/94, 61%) and death (35/94, 37%; overall mortality 7%). In regression analysis, loss to follow up was associated with age 10-14 years (OR 2.38, 95% CI 1.15-4.93, p = 0.02), HIV positivity (OR 3.35, 95% CI 1.41-7.92, p = 0.01), hospitalization (OR 4.14, 95% CI 2.08-8.25, p < 0.001), and living outside of Kampala (OR 2.64, 95% CI 1.47-4.71, p = 0.001). Death was associated with hospitalization (OR 4.57, 95% CI 2.0-10.46, p < 0.001), severe malnutrition (OR 2.98, 95% CI 1.07-8.27, p = 0.04), baseline hepatomegaly (OR 4.11, 95% CI 2.09-8.09, p < 0.001), and living outside of Kampala (OR 2.41, 95% CI 1.17-4.96, p = 0.02).
Empiric treatment of child TB was effective and safe, but treatment success remained below the 90% target. Addressing co-morbidities and improving retention in care may reduce unfavorable outcomes.
儿童结核病(TB)的诊断往往缺乏微生物学证实,需要经验性治疗。经验性治疗的障碍包括对不良结局和不良反应的担忧。因此,我们从乌干达坎帕拉的一家国家转诊医院 2010 年至 2015 年的回顾性队列中确定了经验性 TB 治疗的结局。
根据临床诊断并通过治疗对儿童进行随访。从病历中提取人口统计学、临床数据、结局和任何不良反应。临床改善是定义为儿童完成治疗的良好结局。我们进行逻辑回归分析以评估与失访和死亡相关的因素。
516 名儿童中,中位年龄为 36 个月(IQR 15-73),55%(95%CI 51-60%)为男性,HIV 流行率为 6%(95%CI 4-9%)。大多数(n=422,82%,95%CI 78-85%)有良好结局,没有需要停药的不良反应。最常见的不良结局是失访(57/94,61%)和死亡(35/94,37%;总死亡率 7%)。回归分析显示,失访与 10-14 岁年龄(OR 2.38,95%CI 1.15-4.93,p=0.02)、HIV 阳性(OR 3.35,95%CI 1.41-7.92,p=0.01)、住院(OR 4.14,95%CI 2.08-8.25,p<0.001)和居住在坎帕拉以外(OR 2.64,95%CI 1.47-4.71,p=0.001)有关。死亡与住院(OR 4.57,95%CI 2.0-10.46,p<0.001)、严重营养不良(OR 2.98,95%CI 1.07-8.27,p=0.04)、基线肝肿大(OR 4.11,95%CI 2.09-8.09,p<0.001)和居住在坎帕拉以外(OR 2.41,95%CI 1.17-4.96,p=0.02)有关。
儿童 TB 的经验性治疗是有效且安全的,但治疗成功率仍低于 90%的目标。解决合并症并改善护理保留率可能会降低不良结局的发生。