Neurological Intensive Care Unit, Department of Neurology, Medical University of Innsbruck, Anichstrasse 35, 6020, Innsbruck, Austria.
Medical Informatics, UMIT - University for Health Sciences, Hall, Austria.
Neurocrit Care. 2020 Feb;32(1):135-144. doi: 10.1007/s12028-019-00713-8.
There is no uniform definition for cerebral microdialysis (CMD) probe location with respect to focal brain lesions, and the impact of CMD-probe location on measured molecule concentrations is unclear.
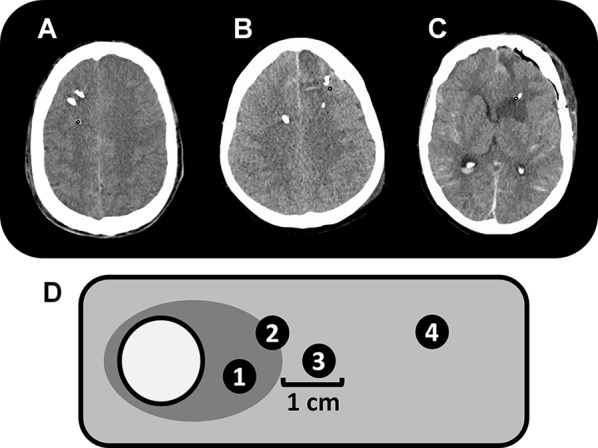
We retrospectively analyzed data of 51 consecutive subarachnoid hemorrhage patients with CMD-monitoring between 2010 and 2016 included in a prospective observational cohort study. Microdialysis probe location was assessed on all brain computed tomography (CT) scans performed during CMD-monitoring and defined as perilesional in the presence of a focal hypodense or hyperdense lesion within a 1-cm radius of the gold tip of the CMD-probe, or otherwise as normal-appearing brain tissue.
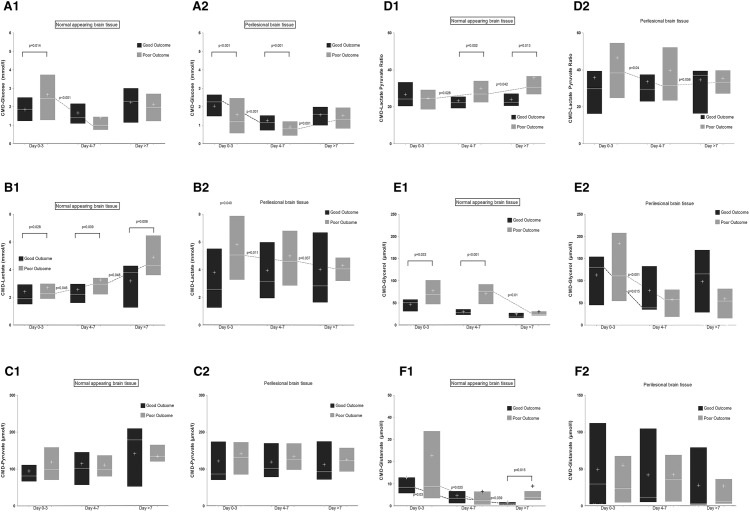
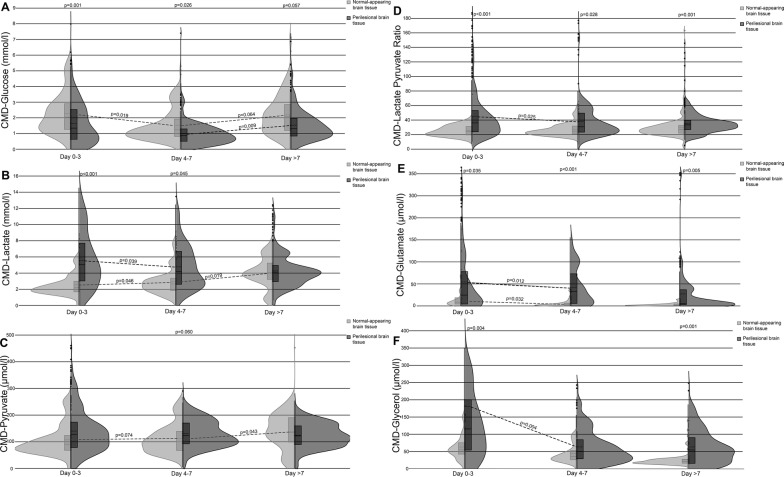
Probe location was detected in normal-appearing brain tissue on 53/143 (37%) and in perilesional location on 90/143 (63%) CT scans. In the perilesional area, CMD-glucose levels were lower (p = 0.003), whereas CMD-lactate (p = 0.002), CMD-lactate-to-pyruvate-ratio (LPR; p < 0.001), CMD-glutamate (p = 0.002), and CMD-glycerol levels (p < 0.001) were higher. Neuroglucopenia (CMD-glucose < 0.7 mmol/l, p = 0.002), metabolic distress (p = 0.002), and mitochondrial dysfunction (p = 0.005) were more common in perilesional compared to normal-appearing brain tissue. Development of new lesions in the proximity of the CMD-probe (n = 13) was associated with a decrease in CMD-glucose levels, evidence of neuroglucopenia, metabolic distress, as well as increasing CMD-glutamate and CMD-glycerol levels. Neuroglucopenia was associated with poor outcome independent of probe location, whereas elevated CMD-lactate, CMD-LPR, CMD-glutamate, and CMD-glycerol levels were only predictive of poor outcome in normal-appearing brain tissue.
Focal brain lesions significantly impact on concentrations of brain metabolites assessed by CMD. With the exception of CMD-glucose, the prognostic value of CMD-derived parameters seems to be higher when assessed in normal-appearing brain tissue. CMD was sensitive to detect the development of new focal lesions in vicinity to the neuromonitoring probe. Probe location should be described in the research reporting brain metabolic changes measured by CMD and integrated in statistical models.
针对局灶性脑病变,脑微透析(CMD)探针位置尚无统一定义,且CMD 探针位置对测量分子浓度的影响尚不清楚。
我们回顾性分析了 2010 年至 2016 年期间连续 51 例蛛网膜下腔出血患者的 CMD 监测数据,这些患者纳入了一项前瞻性观察队列研究。在 CMD 监测期间进行的所有脑计算机断层扫描(CT)检查中评估微透析探针位置,并定义为在 CMD 探针金尖端 1 厘米半径范围内存在局灶性低或高密度病变时为病变周围,否则为正常表现的脑组织。
53/143(37%)例 CT 扫描显示探针位于正常表现的脑组织中,90/143(63%)例 CT 扫描显示探针位于病变周围。在病变周围区域,CMD 葡萄糖水平较低(p=0.003),而 CMD 乳酸(p=0.002)、CMD 乳酸/丙酮酸比值(LPR;p<0.001)、CMD 谷氨酸(p=0.002)和 CMD 甘油水平(p<0.001)较高。与正常表现的脑组织相比,神经糖缺乏症(CMD 葡萄糖<0.7mmol/l,p=0.002)、代谢窘迫(p=0.002)和线粒体功能障碍(p=0.005)更常见于病变周围。CMD 探头附近新发病变的发展(n=13)与 CMD 葡萄糖水平下降、神经糖缺乏症、代谢窘迫以及 CMD 谷氨酸和 CMD 甘油水平升高有关。神经糖缺乏症与不良预后独立相关,而 CMD 乳酸、CMD-LPR、CMD 谷氨酸和 CMD 甘油水平仅在正常表现的脑组织中预测不良预后。
局灶性脑病变显著影响 CMD 评估的脑代谢物浓度。除 CMD 葡萄糖外,CMD 衍生参数的预后价值在正常表现的脑组织中更高。CMD 能够检测到神经监测探头附近新发局灶性病变的发展。在报告 CMD 测量的脑代谢变化的研究中,应描述探针位置并将其纳入统计模型。