Vanderbilt Translational and Clinical Cardiovascular Research Center, Vanderbilt University Medical Center, Nashville, Tennessee; Division of Cardiovascular Medicine, Vanderbilt University Medical Center, Nashville, Tennessee.
Vanderbilt Translational and Clinical Cardiovascular Research Center, Vanderbilt University Medical Center, Nashville, Tennessee; Division of Cardiovascular Medicine, Vanderbilt University Medical Center, Nashville, Tennessee.
J Am Coll Cardiol. 2019 May 7;73(17):2195-2205. doi: 10.1016/j.jacc.2019.01.074.
Circulating biomarkers can facilitate diagnosis and risk stratification for complex conditions such as heart failure (HF). Newer molecular platforms can accelerate biomarker discovery, but they require significant resources for data and sample acquisition.
The purpose of this study was to test a pragmatic biomarker discovery strategy integrating automated clinical biobanking with proteomics.
Using the electronic health record, the authors identified patients with and without HF, retrieved their discarded plasma samples, and screened these specimens using a DNA aptamer-based proteomic platform (1,129 proteins). Candidate biomarkers were validated in 3 different prospective cohorts.
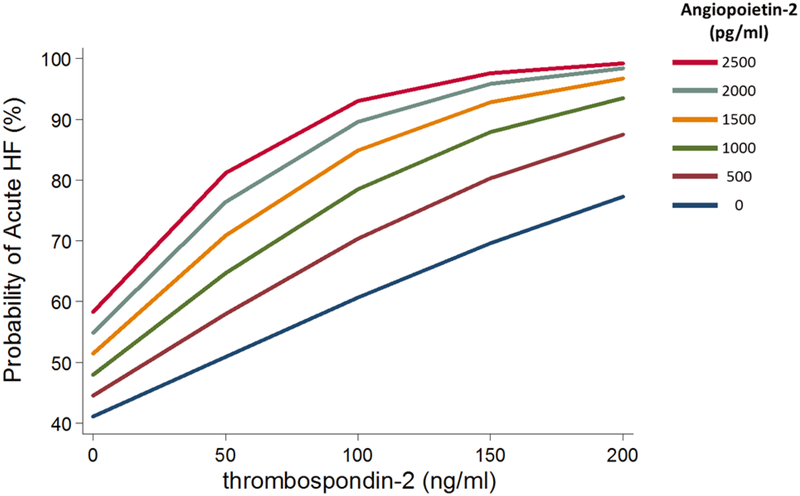
In an automated manner, plasma samples from 1,315 patients (31% with HF) were collected. Proteomic analysis of a 96-patient subset identified 9 candidate biomarkers (p < 4.42 × 10). Two proteins, angiopoietin-2 and thrombospondin-2, were associated with HF in 3 separate validation cohorts. In an emergency department-based registry of 852 dyspneic patients, the 2 biomarkers improved discrimination of acute HF compared with a clinical score (p < 0.0001) or clinical score plus B-type natriuretic peptide (p = 0.02). In a community-based cohort (n = 768), both biomarkers predicted incident HF independent of traditional risk factors and N-terminal pro-B-type natriuretic peptide (hazard ratio per SD increment: 1.35 [95% confidence interval: 1.14 to 1.61; p = 0.0007] for angiopoietin-2, and 1.37 [95% confidence interval: 1.06 to 1.79; p = 0.02] for thrombospondin-2). Among 30 advanced HF patients, concentrations of both biomarkers declined (80% to 84%) following cardiac transplant (p < 0.001 for both).
A novel strategy integrating electronic health records, discarded clinical specimens, and proteomics identified 2 biomarkers that robustly predict HF across diverse clinical settings. This approach could accelerate biomarker discovery for many diseases.
循环生物标志物可促进心力衰竭(HF)等复杂疾病的诊断和风险分层。新型分子平台可加速生物标志物的发现,但它们需要大量的数据和样本采集资源。
本研究旨在测试一种实用的生物标志物发现策略,该策略将自动化临床生物库与蛋白质组学相结合。
作者使用电子病历识别出有和无 HF 的患者,检索其废弃的血浆样本,并使用基于 DNA 适体的蛋白质组学平台(1129 种蛋白质)对这些标本进行筛选。候选生物标志物在 3 个不同的前瞻性队列中进行验证。
以自动化方式收集了 1315 名患者(31%有 HF)的血浆样本。对 96 名患者的亚组进行蛋白质组学分析,鉴定出 9 个候选生物标志物(p < 4.42 × 10)。在 3 个独立的验证队列中,2 种蛋白质(血管生成素 2 和血栓调节蛋白 2)与 HF 相关。在基于急诊科的 852 名呼吸困难患者的登记处,这 2 种生物标志物与临床评分(p < 0.0001)或临床评分加 B 型利钠肽(p = 0.02)相比,改善了急性 HF 的鉴别能力。在社区队列(n = 768)中,2 种生物标志物均独立于传统危险因素和 N 末端脑钠肽前体(每 SD 增加的危险比:血管生成素 2 为 1.35 [95%置信区间:1.14 至 1.61;p = 0.0007],血栓调节蛋白 2 为 1.37 [95%置信区间:1.06 至 1.79;p = 0.02])预测 HF 发生。在 30 名晚期 HF 患者中,心脏移植后 2 种生物标志物的浓度均下降(p < 0.001,均下降 80%至 84%)。
一种将电子病历、废弃的临床标本和蛋白质组学相结合的新策略,鉴定出了 2 种可在不同临床环境中可靠预测 HF 的生物标志物。这种方法可以加速许多疾病的生物标志物发现。