University of Michigan, Ann Arbor, Mich.
Division of Cardiac Surgery, Henry Ford Hospital, Detroit, Mich.
J Thorac Cardiovasc Surg. 2019 Oct;158(4):1073-1080.e4. doi: 10.1016/j.jtcvs.2019.03.042. Epub 2019 Mar 29.
Findings from a large multicenter experience showed that sex influenced the relationship between low nadir hematocrit and increased risk of acute kidney injury after cardiac surgery. We explored whether sex-related differences persisted among patients undergoing isolated coronary artery bypass grafting.
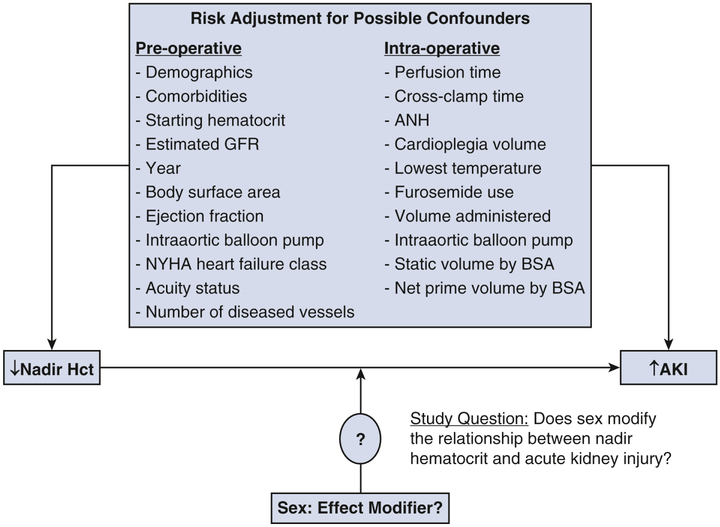
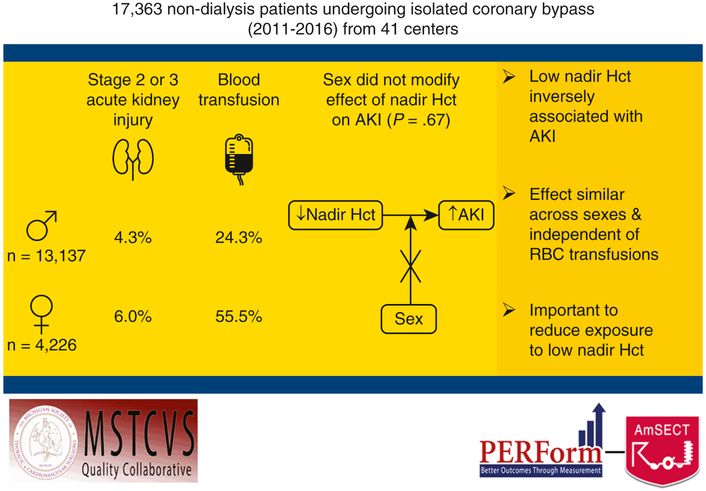
We undertook a prospective, observational study of 17,363 patients without dialysis (13,137 male: 75.7%; 4226 female: 24.3%) undergoing isolated coronary artery bypass grafting between 2011 and 2016 across 41 institutions in the Perfusion Measures and Outcomes registry. Odds ratios between nadir hematocrit and stage 2 or 3 acute kidney injury were calculated, and the interaction of sex with nadir hematocrit was tested. The multivariable, generalized, linear mixed-effect model adjusted for preoperative and intraoperative factors and institution.
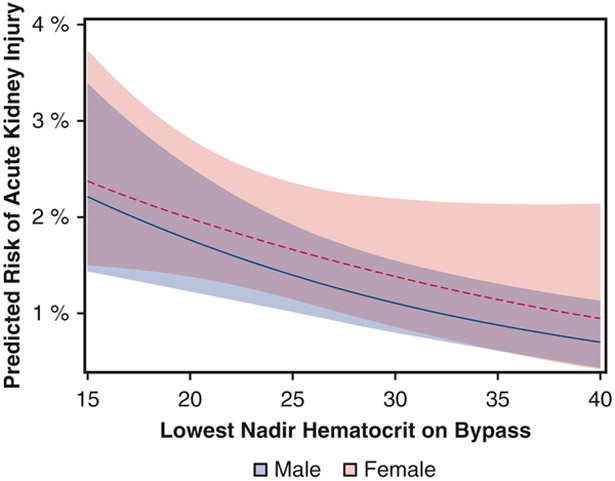
Median nadir hematocrit was 22% among women and 27% among men (P < .001). Women were administered a greater median net prime volume indexed to body surface area (407 vs 363 mL/m) and more red blood cell transfusions (55.5% vs 24.3%; both P < .001). Acute kidney injury was higher among women (6.0% vs 4.3%, P < .001). There was no effect of sex on the relationship between nadir hematocrit and acute kidney injury (P = .67). Low nadir hematocrit was inversely associated with acute kidney injury (adjusted odds ratios per 1-unit increase in nadir hematocrit 0.96; 95% confidence interval, 0.93-0.98); this effect was similar across sexes and independent of red blood cell transfusions.
We found no sex-related differences in the effect of nadir hematocrit on acute kidney injury after isolated coronary artery bypass grafting. However, the strong inverse relationship between anemia and acute kidney injury across sexes suggests the importance of reducing exposure to low nadir hematocrit.
大量多中心研究结果表明,性别会影响心脏手术后低血球压积最低点与急性肾损伤风险增加之间的关系。我们探讨了在接受单纯冠状动脉旁路移植术的患者中,这种性别相关的差异是否仍然存在。
我们对 2011 年至 2016 年间在灌注测量和结果登记处的 41 家机构中接受单纯冠状动脉旁路移植术的 17363 例无透析患者(男性 13137 例,占 75.7%;女性 4226 例,占 24.3%)进行了一项前瞻性、观察性研究。计算了血球压积最低点与 2 期或 3 期急性肾损伤之间的比值比,并检验了性别与血球压积最低点之间的相互作用。多变量、广义线性混合效应模型调整了术前和术中因素以及机构因素。
女性的血球压积最低点中位数为 22%,男性为 27%(P<.001)。女性接受的平均净血球压积指数较高(407 比 363 毫升/米),并且输注的红细胞量也更多(55.5%比 24.3%;均 P<.001)。女性的急性肾损伤发生率更高(6.0%比 4.3%,P<.001)。性别对血球压积最低点与急性肾损伤之间的关系没有影响(P=.67)。低血球压积最低点与急性肾损伤呈负相关(血球压积最低点每增加 1 单位,急性肾损伤的调整比值比为 0.96;95%置信区间,0.93-0.98);这种效应在性别之间是相似的,且独立于红细胞输注。
我们发现,在单纯冠状动脉旁路移植术后,血球压积最低点对急性肾损伤的影响在性别之间没有差异。然而,无论性别如何,贫血与急性肾损伤之间的强烈负相关关系表明,降低接触低血球压积最低点的重要性。