Department of Vascular Surgery, Cardiovascular Center, University of Leipzig, Liebigstr 20, 04103, Leipzig, Germany.
Department of Cardiothoracic and Vascular Surgery, German Heart Center Berlin, Berlin, Germany.
BMC Anesthesiol. 2019 Nov 6;19(1):201. doi: 10.1186/s12871-019-0875-7.
Significant bleeding is a well known complication after cardiac surgical procedures and is associated with worse outcome. Thrombelastometry (ROTEM®) allows point-of-care testing of the coagulation status but only limited data is available yet. The aim was to evaluate the ROTEM®-guided blood component therapy in a randomized trial.
In case of significant postoperative bleeding (> 200 ml/h) following elective isolated or combined cardiac surgical procedures (including 14% re-do procedures and 4% requiring circulatory arrest) patients were randomized to either a 4-chamber ROTEM®-guided blood-component transfusion protocol or received treatment guided by an algorithm based on standard coagulation testing (control). One hundred four patients (mean age: 67.2 ± 10.4 years, mean log. EuroSCORE 7.0 ± 8.8%) met the inclusion criteria. Mean CPB-time was 112.1 ± 55.1 min., mean cross-clamp time 72.5 ± 39.9 min.
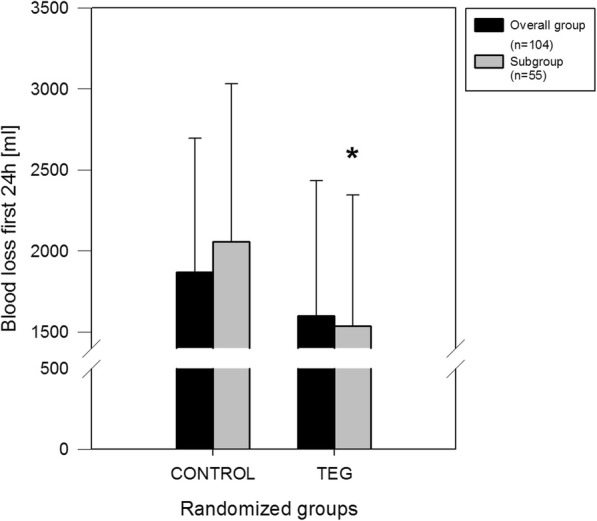
Baseline demographics were comparable in both groups. Overall there was no significant difference in transfusion requirements regarding red blood cells, platelets, plasma, fibrinogen or pooled factors and the re-thoracotomy rate was comparable (ROTEM®: 29% vs. control: 25%). However, there was a trend towards less 24-h drainage loss visible in the ROTEM®-group (ROTEM®: 1599.1 ± 834.3 ml vs. control: 1867.4 ± 827.4 ml; p = 0.066). In the subgroup of patients with long CPB-times (> 115 min.; n = 55) known to exhibit an increased risk for diffuse coagulopathy ROTEM®-guided treatment resulted in a significantly lower 24-h drainage loss (ROTEM®: 1538.2 ± 806.4 ml vs. control: 2056.8 ± 974.5 ml; p = 0.032) and reduced 5-year mortality (ROTEM®: 0% vs. control: 15%; p = 0.03).
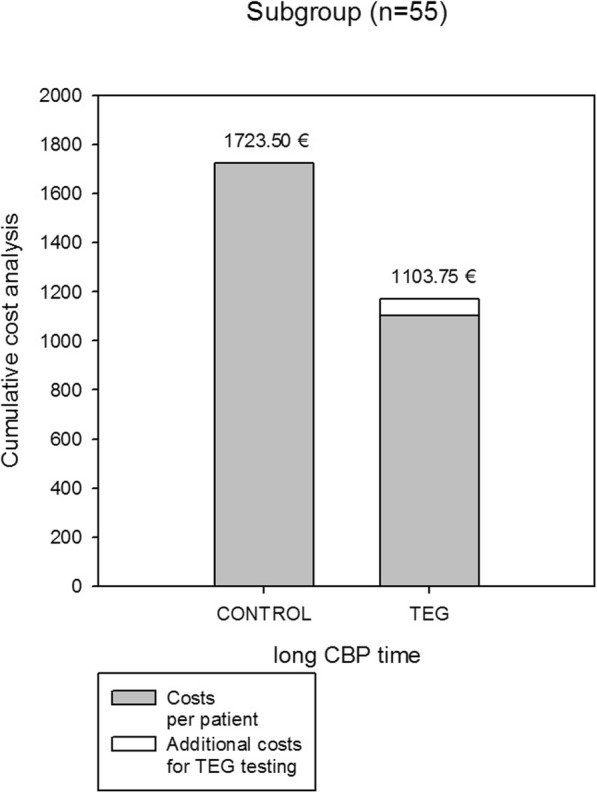
In case of postoperative bleeding following cardiac surgical procedures a treatment algorithm based on "point-of-care" 4-chamber ROTEM® seems to be at least as effective as standard therapy. In patients with long CPB-times ROTEM®-guided treatment may result in less bleeding, a marked reduction in costs and long-term mortality.
German Clinical Trials Register, TRN: DRKS00017367 , date of registration: 05.06.2019, 'retrospectively registered'.
心脏手术后大量出血是一种众所周知的并发症,与较差的预后相关。血栓弹性描记术(ROTEM®)允许即时检测凝血状态,但目前可用的数据有限。目的是在随机试验中评估 ROTEM®指导的血液成分治疗。
在择期进行的心脏外科手术(包括 14%的再次手术和 4%需要体外循环的手术)后出现明显术后出血(>200ml/h)的情况下,患者被随机分配至四腔室 ROTEM®指导的血液成分输血方案或接受基于标准凝血检测的算法指导的治疗(对照组)。104 名患者(平均年龄:67.2±10.4 岁,平均 log.EuroSCORE7.0±8.8%)符合纳入标准。CPB 时间平均为 112.1±55.1 分钟,平均体外循环夹闭时间为 72.5±39.9 分钟。
两组患者的基线特征无显著差异。总体而言,两组在红细胞、血小板、血浆、纤维蛋白原或混合因素的输血需求方面没有显著差异,开胸再探查率相当(ROTEM®:29%vs.对照组:25%)。然而,在 ROTEM®组中,24 小时引流损失量有减少的趋势(ROTEM®:1599.1±834.3ml vs.对照组:1867.4±827.4ml;p=0.066)。在已知存在弥漫性凝血障碍风险增加的 CPB 时间较长(>115 分钟;n=55)的患者亚组中,ROTEM®指导的治疗导致 24 小时引流损失量显著降低(ROTEM®:1538.2±806.4ml vs.对照组:2056.8±974.5ml;p=0.032)和降低 5 年死亡率(ROTEM®:0%vs.对照组:15%;p=0.03)。
在心脏手术后出现术后出血的情况下,基于“即时检测”四腔室 ROTEM®的治疗方案似乎至少与标准治疗一样有效。在 CPB 时间较长的患者中,ROTEM®指导的治疗可能会导致更少的出血、显著降低成本和长期死亡率。
德国临床试验注册处,TRN:DRKS00017367,登记日期:2019 年 6 月 5 日,“回顾性登记”。