Zborovski Stephen, Palmert Mark R, Harrington Jennifer
Division of Endocrinology, Department of Pediatrics, Hospital for Sick Children, University of Toronto, Toronto, Canada.
J Endocr Soc. 2019 Mar 28;3(5):1022-1030. doi: 10.1210/js.2018-00390. eCollection 2019 May 1.
In children with isolated growth hormone (GH) deficiency (GHD), routine biochemical screening for multiple pituitary hormone deficiencies (MPHD) and adverse effects related to growth hormone (GH) treatment are frequently performed. More evidence is needed to support this practice.
To evaluate the rate of development of MPHD among children initially diagnosed with isolated GHD and to assess the utility of screening tests to identify complications of GH therapy.
Retrospective analysis of subjects treated with GH since 2005. For the first objective, only subjects diagnosed with GHD were included. Subjects were excluded if GHD was associated with an acquired disorder or condition known to be associated with pituitary abnormalities. For the second objective, other GH-treated diagnoses were included.
A total of 328 subjects (171 with GHD, 154 with idiopathic short stature, and three with deficiency).
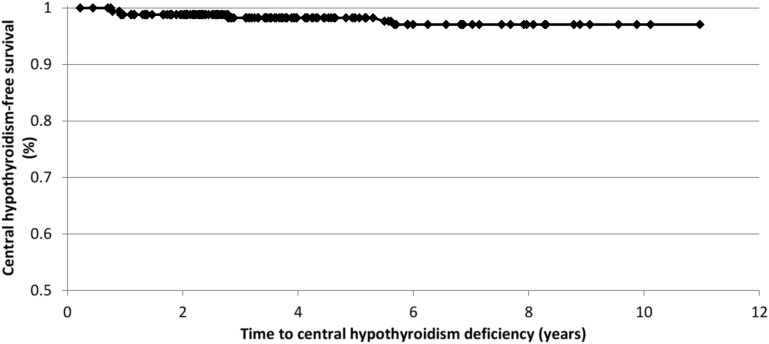
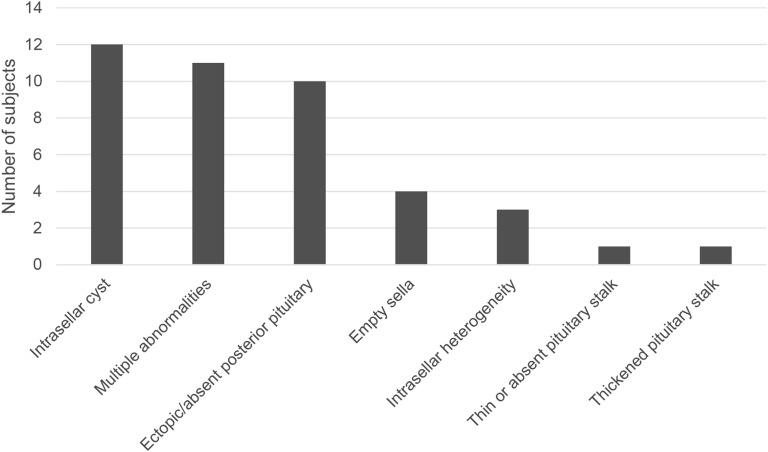
In subjects with isolated GHD, MPHD was diagnosed in seven (4.2%) after a mean of 35.4 months (range, 9.4 to 68.0). Sex, age at diagnosis, duration of GH, and peak stimulated GH levels were not associated with developing MPHD. Among subjects with an MRI abnormality, 13.9% developed MPHD (OR, 6.3; 95% CI, 1.2 to 33.7). In the entire cohort, three subjects (0.9%) developed dysglycemia, and no subject had persistently abnormal liver or renal function tests.
There is a limited role for routine biochemical screening for MPHD in children with idiopathic isolated GHD or for adverse effects in otherwise healthy children. Routine biochemical screening for MPHD should be limited to those with an abnormal MRI.
在孤立性生长激素(GH)缺乏症(GHD)患儿中,常进行多项垂体激素缺乏症(MPHD)的常规生化筛查以及与生长激素(GH)治疗相关的不良反应筛查。需要更多证据来支持这种做法。
评估最初诊断为孤立性GHD的儿童中MPHD的发生率,并评估筛查试验在识别GH治疗并发症方面的效用。
对2005年以来接受GH治疗的受试者进行回顾性分析。对于第一个目标,仅纳入诊断为GHD的受试者。如果GHD与已知与垂体异常相关的后天性疾病或状况相关,则将受试者排除。对于第二个目标,纳入其他接受GH治疗的诊断。
总共328名受试者(171名GHD患者,154名特发性身材矮小患者,3名其他缺乏症患者)。
在孤立性GHD受试者中,平均35.4个月(范围9.4至68.0)后,7名(4.2%)被诊断为MPHD。性别、诊断时年龄、GH治疗持续时间和刺激后GH峰值水平与发生MPHD无关。在MRI异常的受试者中,13.9%发生了MPHD(比值比,6.3;95%置信区间,1.2至33.7)。在整个队列中,3名受试者(0.9%)出现血糖异常,没有受试者的肝功能或肾功能检查持续异常。
对于特发性孤立性GHD儿童进行MPHD常规生化筛查或对其他健康儿童进行不良反应筛查的作用有限。MPHD的常规生化筛查应限于MRI异常的儿童。