Pediatric Endocrinology-Diabetology Department, Reference Center for Growth and Development Endocrine Diseases, Robert Debré University Hospital, Assistance Publique-Hôpitaux de Paris, Université de Paris, 48 Bd Sérurier, 75019, Paris, France.
Banque Nationale de Données Maladies Rares, DSI-I&D, APHP, Paris, France.
Orphanet J Rare Dis. 2021 Nov 4;16(1):469. doi: 10.1186/s13023-021-02099-3.
For chronic congenital endocrine conditions, age at diagnosis is a key issue with implications for optimal management and psychological concerns. These conditions are associated with an increase in the risk of comorbid conditions, particularly as it concerns growth, pubertal development and fertility potential. Clinical presentation and severity depend on the disorder and the patient's age, but diagnosis is often late.
To evaluate age at diagnosis for the most frequent congenital endocrine diseases affecting growth and/or development.
This observational cohort study included all patients (n = 4379) with well-defined chronic congenital endocrine diseases-non-acquired isolated growth hormone deficiency (IGHD), isolated congenital hypogonadotropic hypogonadism (ICHH), ectopic neurohypophysis (NH), Turner syndrome (TS), McCune-Albright syndrome (MAS), complete androgen insensitivity syndrome (CAIS) and gonadal dysgenesis (GD)-included in the database of a single multisite reference center for rare endocrine growth and developmental disorders, over a period of 14 years. Patients with congenital hypothyroidism and adrenal hyperplasia were excluded as they are generally identified during neonatal screening.
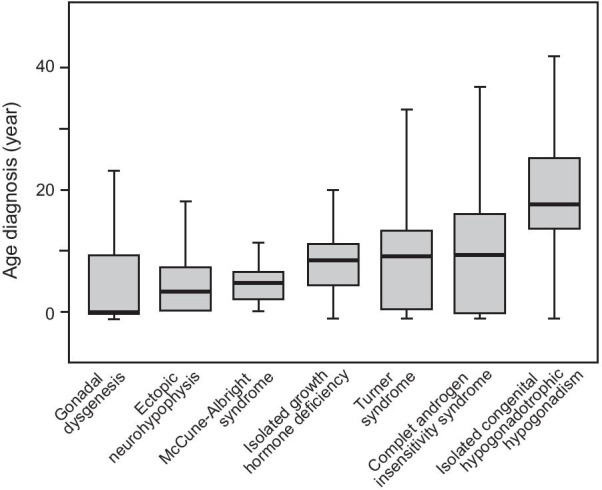
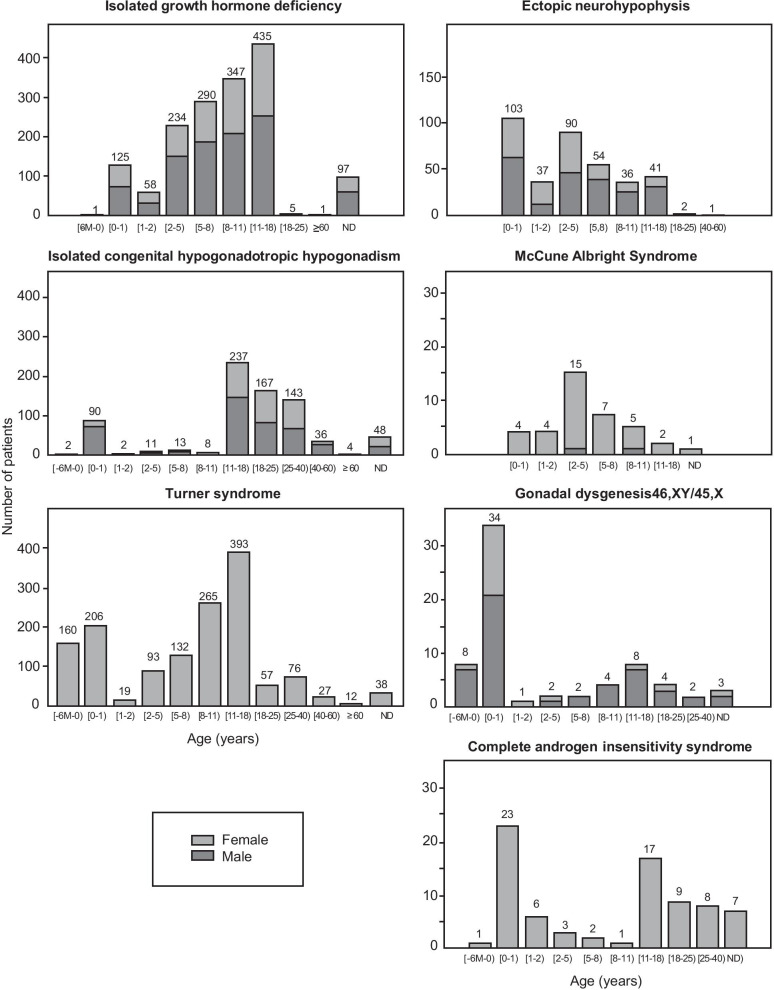
Median age at diagnosis depended on the disease: first year of life for GD, before the age of five years for ectopic NH and MAS, 8-10 years for IGHD, TS (11% diagnosed antenatally) and CAIS and 17.4 years for ICHH. One third of the patients were diagnosed before the age of five years. Diagnosis occurred in adulthood in 22% of cases for CAIS, 11.6% for TS, 8.8% for GD, 0.8% for ectopic NH, and 0.4% for IGHD. A male predominance (2/3) was observed for IGHD, ectopic NH, ICHH and GD.
The early recognition of growth/developmental failure during childhood is essential, to reduce time-to-diagnosis and improve outcomes.
对于慢性先天性内分泌疾病,诊断时的年龄是一个关键问题,这涉及到最佳管理和心理问题。这些疾病与合并症的风险增加有关,特别是在生长、青春期发育和生育潜力方面。临床表现和严重程度取决于疾病和患者的年龄,但诊断往往较晚。
评估影响生长和/或发育的最常见先天性内分泌疾病的诊断年龄。
本观察性队列研究纳入了数据库中所有患有明确慢性先天性内分泌疾病的患者(n=4379),这些疾病包括非获得性孤立性生长激素缺乏症(IGHD)、孤立性先天性低促性腺激素性性腺功能减退症(ICHH)、异位神经垂体(NH)、特纳综合征(TS)、McCune-Albright 综合征(MAS)、完全雄激素不敏感综合征(CAIS)和性腺发育不全(GD),这些患者均来自单一多中心罕见内分泌生长和发育障碍参考中心,研究时间为 14 年。由于先天性甲状腺功能减退症和肾上腺增生症患者通常在新生儿筛查中被发现,因此排除了这些患者。
根据疾病的不同,中位诊断年龄有所不同:GD 的诊断年龄为 1 岁以下,异位 NH 和 MAS 的诊断年龄为 5 岁以下,IGHD、TS(11%在产前诊断)和 CAIS 的诊断年龄为 8-10 岁,ICHH 的诊断年龄为 17.4 岁。三分之一的患者在 5 岁之前被诊断。22%的 CAIS 患者、11.6%的 TS 患者、8.8%的 GD 患者、0.8%的异位 NH 患者和 0.4%的 IGHD 患者在成年后被诊断。IGHD、异位 NH、ICHH 和 GD 患者中男性占 2/3。
在儿童时期早期识别生长/发育障碍至关重要,这可以减少诊断时间并改善预后。