Division of Infectious Diseases, Department of Medicine, University of California, Los Angeles, California, United States of America.
Department of Mechanical and Aerospace Engineering, University of California, Los Angeles, California, United States of America.
PLoS One. 2019 May 10;14(5):e0215607. doi: 10.1371/journal.pone.0215607. eCollection 2019.
Shorter, more effective treatments for tuberculosis (TB) are urgently needed. While many TB drugs are available, identification of the best regimens is challenging because of the large number of possible drug-dose combinations. We have found consistently that responses of cells or whole animals to drug-dose stimulations fit a parabolic response surface (PRS), allowing us to identify and optimize the best drug combinations by testing only a small fraction of the total search space. Previously, we used PRS methodology to identify three regimens (PRS Regimens I-III) that in murine models are much more effective than the standard regimen used to treat TB. However, PRS Regimens I and II are unsuitable for treating drug-resistant TB and PRS Regimen III includes an experimental drug. Here, we use PRS methodology to identify from an expanded pool of drugs new highly effective near-universal drug regimens comprising only approved drugs.
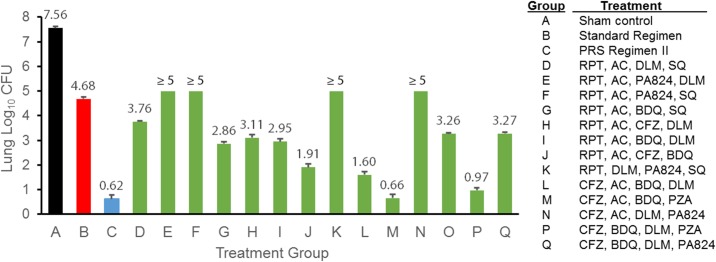
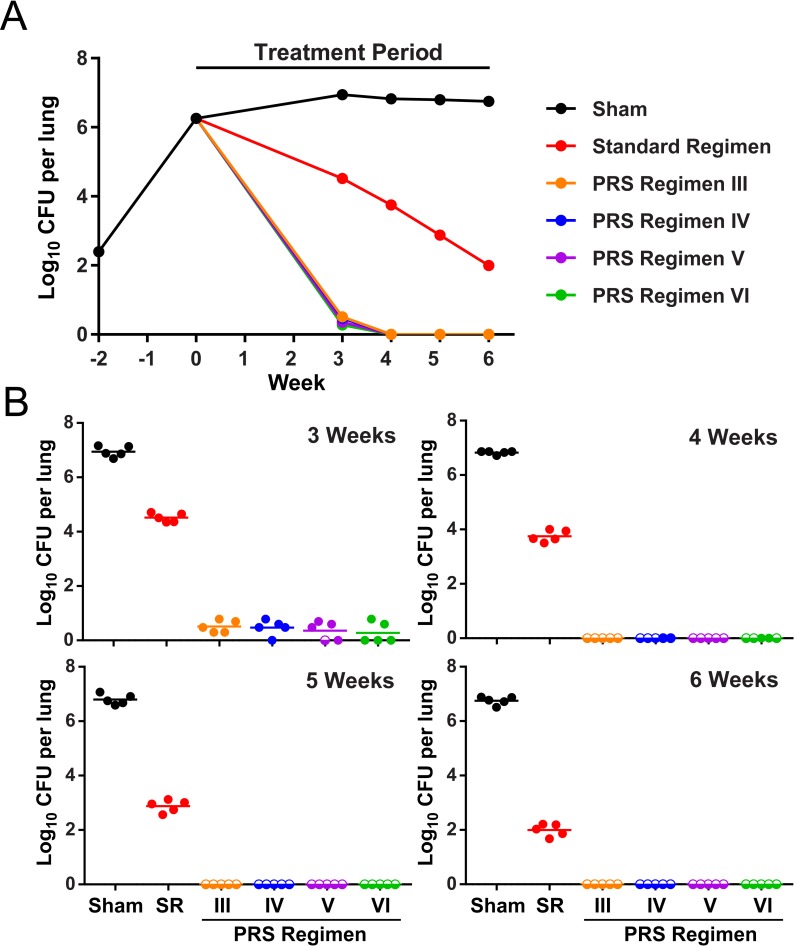
We evaluated combinations of 15 different drugs in a human macrophage TB model and identified the most promising 4-drug combinations. We then tested 14 of these combinations in Mycobacterium tuberculosis-infected BALB/c mice and chose for PRS dose optimization and further study the two most potent regimens, designated PRS Regimens IV and V, consisting of clofazimine (CFZ), bedaquiline (BDQ), pyrazinamide (PZA), and either amoxicillin/clavulanate (AC) or delamanid (DLM), respectively. We then evaluated the efficacy in mice of optimized PRS Regimens IV and V, as well as a 3-drug regimen, PRS Regimen VI (CFZ, BDQ, and PZA), and compared their efficacy to PRS Regimen III (CFZ, BDQ, PZA, and SQ109), previously shown to reduce the time to achieve relapse-free cure in mice by 80% compared with the Standard Regimen (isoniazid, rifampicin, PZA, and ethambutol). Efficacy measurements included early bactericidal activity, time to lung sterilization, and time to relapse-free cure. PRS Regimens III-VI all rapidly sterilized the lungs and achieved relapse-free cure in 3 weeks (PRS Regimens III, V, and VI) or 5 weeks (PRS Regimen IV). In contrast, mice treated with the Standard Regimen still had high numbers of bacteria in their lungs after 6-weeks treatment and none achieved relapse-free cure in this time-period.
We have identified three new regimens that rapidly sterilize the lungs of mice and dramatically shorten the time required to achieve relapse-free cure. All mouse drug doses in these regimens extrapolate to doses that are readily achievable in humans. Because PRS Regimens IV and V contain only one first line drug (PZA) and exclude fluoroquinolones and aminoglycosides, they should be effective against most TB cases that are multidrug resistant (MDR-TB) and many that are extensively drug-resistant (XDR-TB). Hence, these regimens have potential to shorten dramatically the time required for treatment of both drug-sensitive and drug-resistant TB. If clinical trials confirm that these regimens dramatically shorten the time required to achieve relapse-free cure in humans, then this radically shortened treatment has the potential to improve treatment compliance, decrease the emergence of drug resistance, and decrease the healthcare burden of treating both drug-sensitive and drug-resistant TB.
目前急需开发更短、更有效的结核病(TB)治疗方法。尽管有许多治疗结核病的药物,但由于可能的药物剂量组合数量众多,因此确定最佳方案具有挑战性。我们发现细胞或整个动物对药物剂量刺激的反应始终符合抛物线反应表面(PRS),这使我们能够通过仅测试总搜索空间的一小部分来识别和优化最佳药物组合。此前,我们使用 PRS 方法学鉴定了三种方案(PRS 方案 I-III),在小鼠模型中,这三种方案比用于治疗结核病的标准方案有效得多。然而,PRS 方案 I 和 II 不适合治疗耐多药结核病,PRS 方案 III 包含一种实验性药物。在这里,我们使用 PRS 方法学从扩展的药物库中确定了新的高度有效的通用药物方案,这些方案仅包含已批准的药物。
我们在人类巨噬细胞结核病模型中评估了 15 种不同药物的组合,并确定了最有前途的 4 种药物组合。然后,我们在感染结核分枝杆菌的 BALB/c 小鼠中测试了其中的 14 种组合,并选择了两种最有效的方案 PRS 方案 IV 和 V 进行 PRS 剂量优化和进一步研究,这两种方案分别由氯法齐明(CFZ)、贝达喹啉(BDQ)、吡嗪酰胺(PZA)和阿莫西林/克拉维酸(AC)或德拉马尼(DLM)组成。然后,我们评估了优化的 PRS 方案 IV 和 V 以及 3 种药物方案 PRS 方案 VI(CFZ、BDQ 和 PZA)在小鼠中的疗效,并将其与 PRS 方案 III(CFZ、BDQ、PZA 和 SQ109)进行比较,此前已证明与标准方案(异烟肼、利福平、PZA 和乙胺丁醇)相比,PRS 方案 III 可将小鼠达到无复发治愈的时间缩短 80%。疗效测量包括早期杀菌活性、肺部杀菌时间和无复发治愈时间。PRS 方案 III-VI 均迅速使肺部无菌,并在 3 周(PRS 方案 III、V 和 VI)或 5 周(PRS 方案 IV)内实现无复发治愈。相比之下,用标准方案治疗的小鼠在 6 周治疗后肺部仍有大量细菌,在此期间没有无复发治愈。
我们已经确定了三种新方案,这些方案可迅速使小鼠肺部无菌,并大大缩短达到无复发治愈所需的时间。这些方案中的所有小鼠药物剂量都可以外推到人类中容易达到的剂量。由于 PRS 方案 IV 和 V 仅包含一种一线药物(PZA),并排除了氟喹诺酮类和氨基糖苷类药物,因此它们应该对大多数耐多药结核病(MDR-TB)和许多广泛耐药结核病(XDR-TB)有效。因此,这些方案有可能大大缩短治疗耐多药和耐多药结核病所需的时间。如果临床试验证实这些方案可大大缩短人类达到无复发治愈所需的时间,那么这种大大缩短的治疗方案有可能提高治疗依从性,减少药物耐药性的出现,并减轻治疗耐多药和耐多药结核病的医疗保健负担。