Department of Surgery, Ashikaga Red Cross Hospital, Tochigi 326-0843, Japan.
World J Gastroenterol. 2019 Apr 28;25(16):1975-1985. doi: 10.3748/wjg.v25.i16.1975.
Emergency surgical resection is a standard treatment for right-sided malignant colonic obstruction; however, the procedure is associated with high rates of mortality and morbidity. Although a bridge to surgery can be created to obviate the need for emergency surgery, its effects on long-term outcomes and the most practical management strategies for right-sided malignant colonic obstruction remain unclear.
To determine the appropriate management approach for right-sided malignant colonic obstruction.
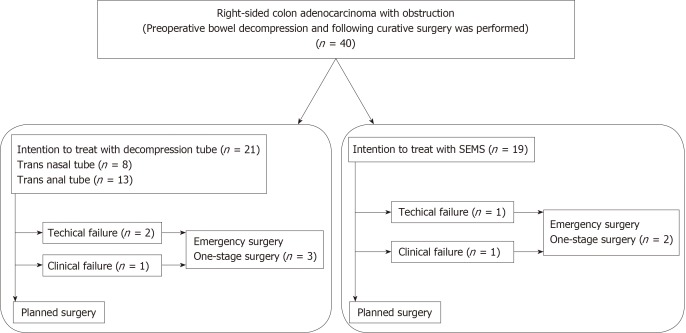
Forty patients with right-sided malignant colonic obstruction who underwent curative resection from January 2007 to April 2017 were included in the study. We compared the perioperative and long-term outcomes of patients who received bridges to surgery established using decompression tubes and those created using self-expandable metallic stents (SEMS). The primary outcome was the overall survival duration (OS) and the secondary endpoints were the disease-free survival (DFS) duration and the preoperative and postoperative morbidity rates. Analysis was performed on an intention-to-treat basis.
There were 21 patients in the decompression tube group and 19 in the SEMS group. There were no significant differences in the perioperative morbidity rates of the two groups. The OS rate was significantly higher in the decompression tube group than in the SEMS group (5-year OS rate; decompression tube 79.5%, SEMS 32%, = 0.043). Multivariate analysis revealed that the bridge to surgery using a decompression tube was significantly associated with the OS (hazard ratio, 17.41; = 0.004). The 3-year DFS rate was significantly higher in the decompression tube group than in the SEMS group (68.9% 45.9%; log-rank test, = 0.032). A propensity score-adjusted analysis also demonstrated that the prognosis was significantly better in the decompression tube group than in the SEMS group.
The bridge to surgery using trans-nasal and trans-anal decompression tubes for right-sided malignant colonic obstruction is safe and may improve long-term outcomes.
急诊手术切除是治疗右侧恶性结肠梗阻的标准方法;然而,该手术与较高的死亡率和发病率相关。尽管可以创建桥接手术以避免急诊手术的需要,但对于右侧恶性结肠梗阻,其对长期结果的影响以及最实用的管理策略仍不清楚。
确定右侧恶性结肠梗阻的适当管理方法。
纳入了 2007 年 1 月至 2017 年 4 月期间接受根治性切除术的 40 例右侧恶性结肠梗阻患者。我们比较了使用减压管和自膨式金属支架(SEMS)建立桥接手术的患者的围手术期和长期结果。主要结局是总生存时间(OS),次要结局是无病生存(DFS)时间以及术前和术后发病率。分析基于意向治疗进行。
减压管组有 21 例患者,SEMS 组有 19 例患者。两组的围手术期发病率无显著差异。减压管组的 OS 率明显高于 SEMS 组(5 年 OS 率;减压管组 79.5%,SEMS 组 32%,=0.043)。多变量分析显示,使用减压管进行桥接手术与 OS 显著相关(危险比,17.41;=0.004)。减压管组的 3 年 DFS 率明显高于 SEMS 组(68.9% 45.9%;对数秩检验,=0.032)。倾向评分调整分析也表明,减压管组的预后明显优于 SEMS 组。
对于右侧恶性结肠梗阻,经鼻和经肛门减压管桥接手术是安全的,可能改善长期结果。