Luxardo Rosario, Kramer Anneke, González-Bedat Maria Carlota, Massy Ziad A, Jager Kitty J, Rosa-Diez Guillermo, Noordzij Marlies
Executive Board of the Latin American Dialysis and Transplant Registry (RLADTR), and Latin American Dialysis and Transplant Society (SLANH), Panama City, Panama.
European Renal Association-European Dialysis and Transplant Association Registry, Department of Medical Informatics, Academic Medical Center, University of Amsterdam, Amsterdam Public Health Research Institute, Amsterdam, the Netherlands.
Rev Panam Salud Publica. 2018 Sep 7;42:e87. doi: 10.26633/RPSP.2018.87. eCollection 2018.
To compare the epidemiology of renal replacement therapy (RRT) for end-stage renal disease (ESRD) in Latin America and Europe, as well as to study differences in macroeconomic indicators, demographic and clinical patient characteristics, mortality rates, and causes of death between these two populations.
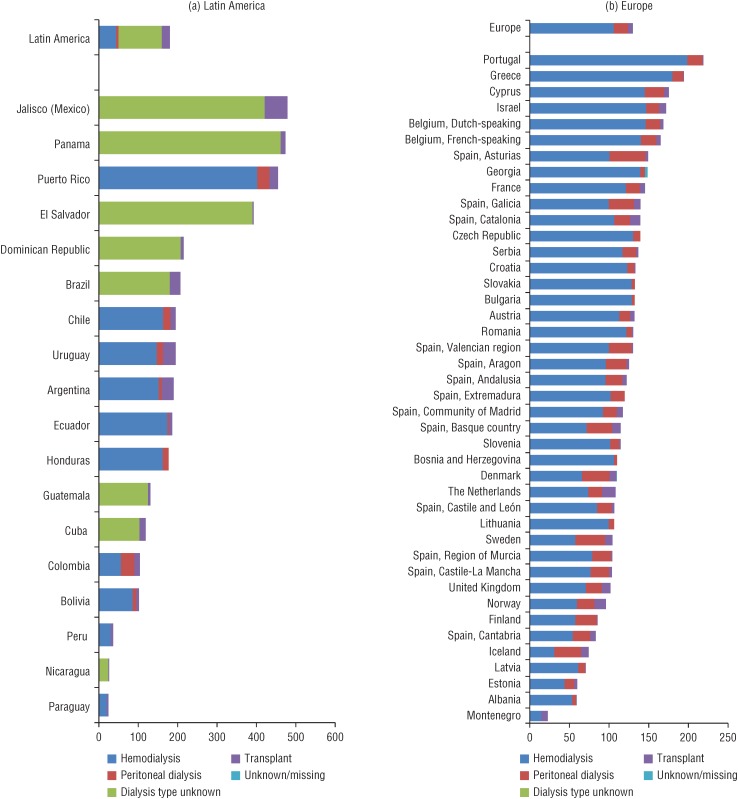
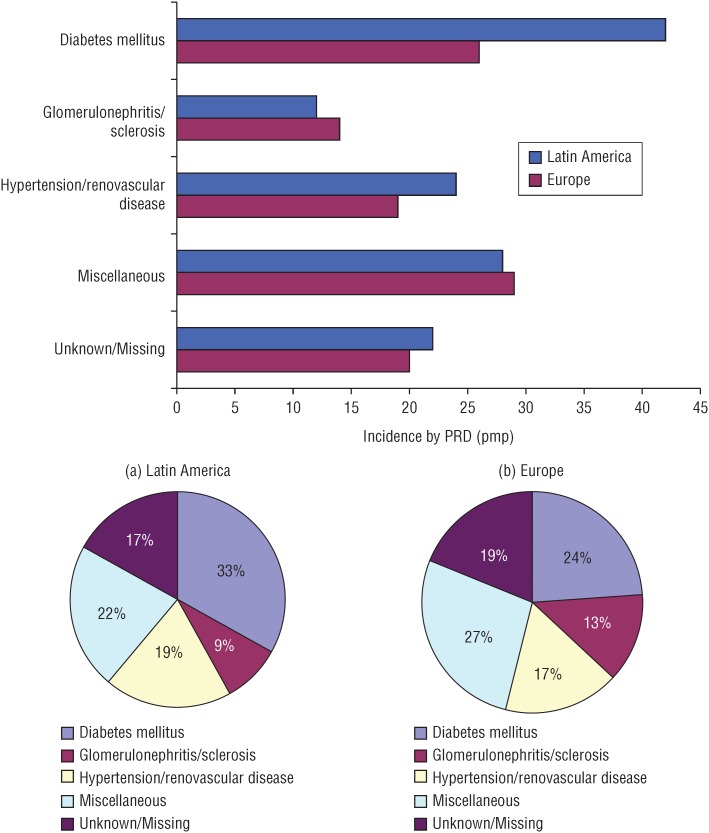
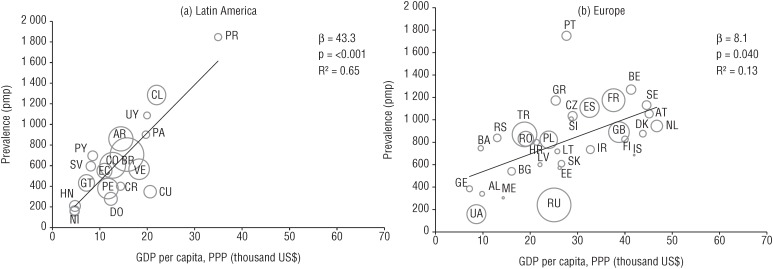
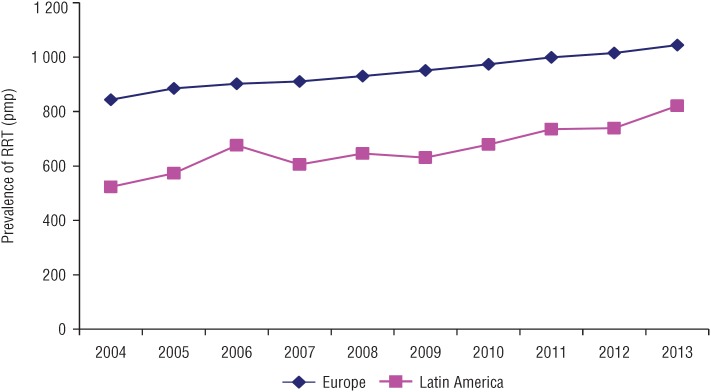
We used data from 20 Latin American and 49 European national and subnational renal registries that had provided data to the Latin American Dialysis and Renal Transplant Registry (RLADTR) and the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) Registry, respectively. The incidence and prevalence of RRT in 2013 were calculated per million population (pmp), overall and by subcategories of age, sex, primary renal disease, and treatment modality. The correlation between gross domestic product and the prevalence of RRT was analyzed using linear regression. Trends in the prevalence of RRT between 2004 and 2013 were assessed using Joinpoint regression analysis.
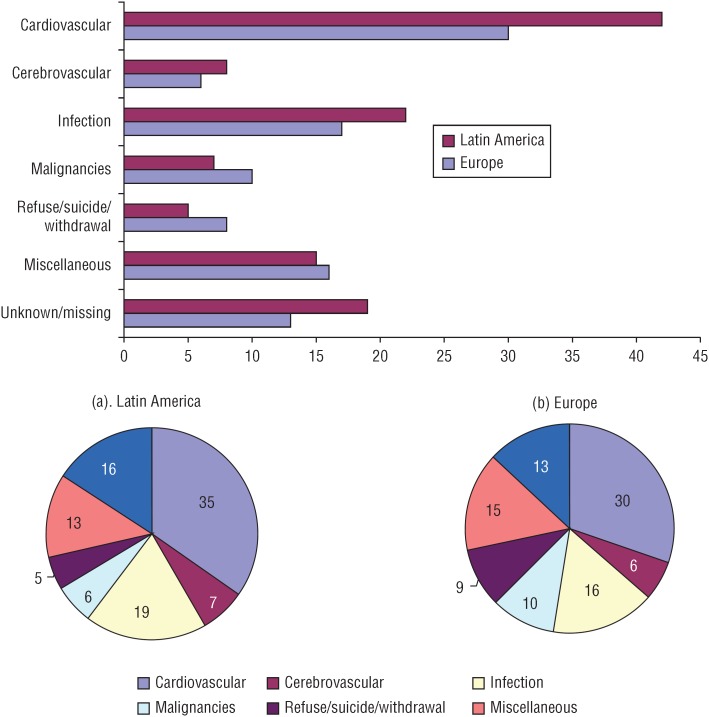
In 2013, the overall incidence at day 91 after the onset of RRT was 181 pmp for Latin American countries and 130 pmp for European countries. The overall prevalence was 660 pmp for Latin America and 782 pmp for Europe. In the Latin American countries, the annual increase in the prevalence averaged 4.0% (95% confidence interval (CI): 2.5%-5.6%) from 2004 to 2013, while the European countries showed an average annual increase of 2.2% (95% CI: 2.0%-2.4%) for the same time period. The crude mortality rate was higher in Latin America than in Europe (112 versus 100 deaths per 1 000 patient-years), and cardiovascular disease was the main cause of death in both of those regions.
There are considerable differences between Latin America and Europe in the epidemiology of RRT for ESRD. Further research is needed to explore the reasons for these differences.
比较拉丁美洲和欧洲终末期肾病(ESRD)的肾脏替代治疗(RRT)流行病学,以及研究这两个人口群体在宏观经济指标、人口统计学和临床患者特征、死亡率及死亡原因方面的差异。
我们使用了分别向拉丁美洲透析和肾脏移植登记处(RLADTR)及欧洲肾脏协会 - 欧洲透析和移植协会(ERA - EDTA)登记处提供数据的20个拉丁美洲国家和49个欧洲国家及次国家级肾脏登记处的数据。计算了2013年每百万人口(pmp)的RRT发病率和患病率,总体情况以及按年龄、性别、原发性肾脏疾病和治疗方式的子类别进行计算。使用线性回归分析国内生产总值与RRT患病率之间的相关性。使用Joinpoint回归分析评估2004年至2013年期间RRT患病率的趋势。
2013年,RRT开始后第91天的总体发病率,拉丁美洲国家为181 pmp,欧洲国家为130 pmp。总体患病率拉丁美洲为660 pmp,欧洲为782 pmp。在拉丁美洲国家,2004年至2013年期间患病率的年平均增长率为4.0%(95%置信区间(CI):2.5% - 5.6%),而同期欧洲国家的年平均增长率为2.2%(95% CI:2.0% - 2.4%)。拉丁美洲的粗死亡率高于欧洲(每1000患者年112例死亡对100例死亡),且心血管疾病是这两个地区的主要死亡原因。
拉丁美洲和欧洲在ESRD的RRT流行病学方面存在相当大的差异。需要进一步研究以探讨这些差异的原因。