Department of Health Research Methods, Evidence, and Impact, McMaster University, McMaster Innovation Park, 175 Longwood Road South, Hamilton, ON, L8P 0A1, Canada.
Department of Family Medicine, University of Alberta, 6-10 University Terrace, Edmonton, AB, T6G 2T4, Canada.
BMC Health Serv Res. 2019 May 16;19(1):313. doi: 10.1186/s12913-019-4149-3.
Most studies that examine comorbidity and its impact on health service utilization focus on a single index-condition and are published in disease-specific journals, which limit opportunities to identify patterns across conditions/disciplines. These comparisons are further complicated by the impact of using different study designs, multimorbidity definitions and data sources. The aim of this paper is to share insights on multimorbidity and associated health services use and costs by reflecting on the common patterns across 3 parallel studies in distinct disease cohorts (diabetes, dementia, and stroke) that used the same study design and were conducted in the same health jurisdiction over the same time period.
We present findings that lend to broader Insights regarding multimorbidity based on the relationship between comorbidity and health service use and costs seen across three distinct disease cohorts. These cohorts were originally created using multiple linked administrative databases to identify community-dwelling residents of Ontario, Canada with one of diabetes, dementia, or stroke in 2008 and each was followed for health service use and associated costs.
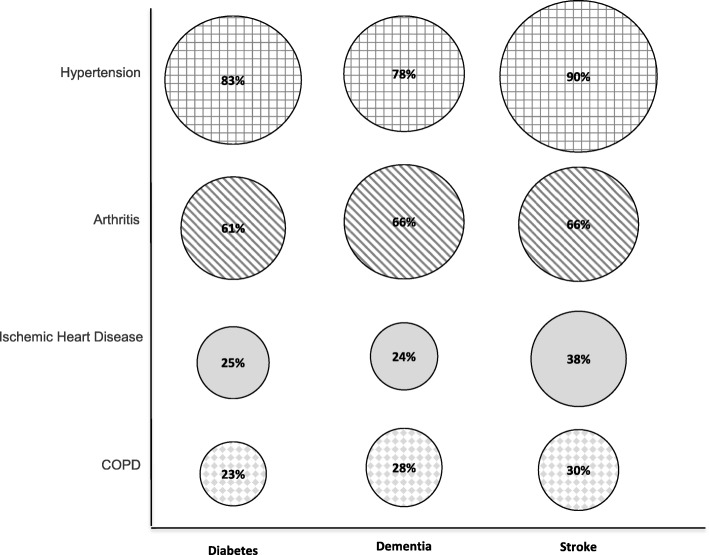
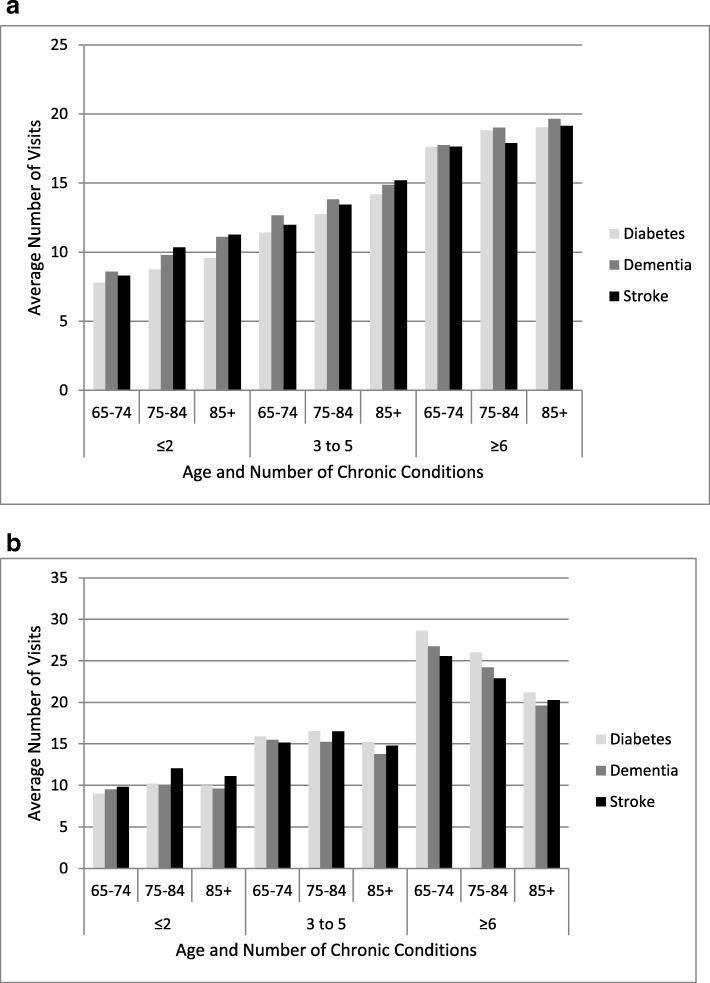
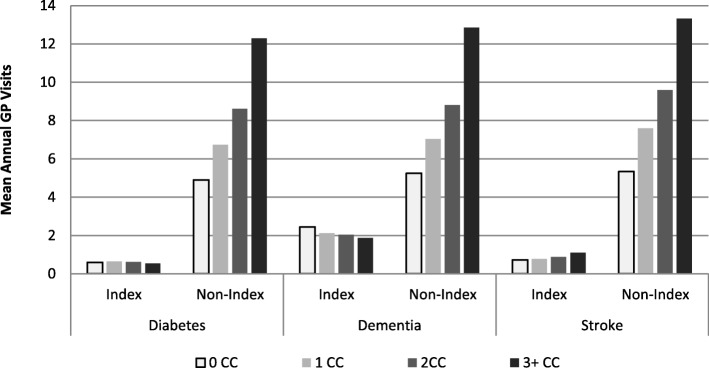
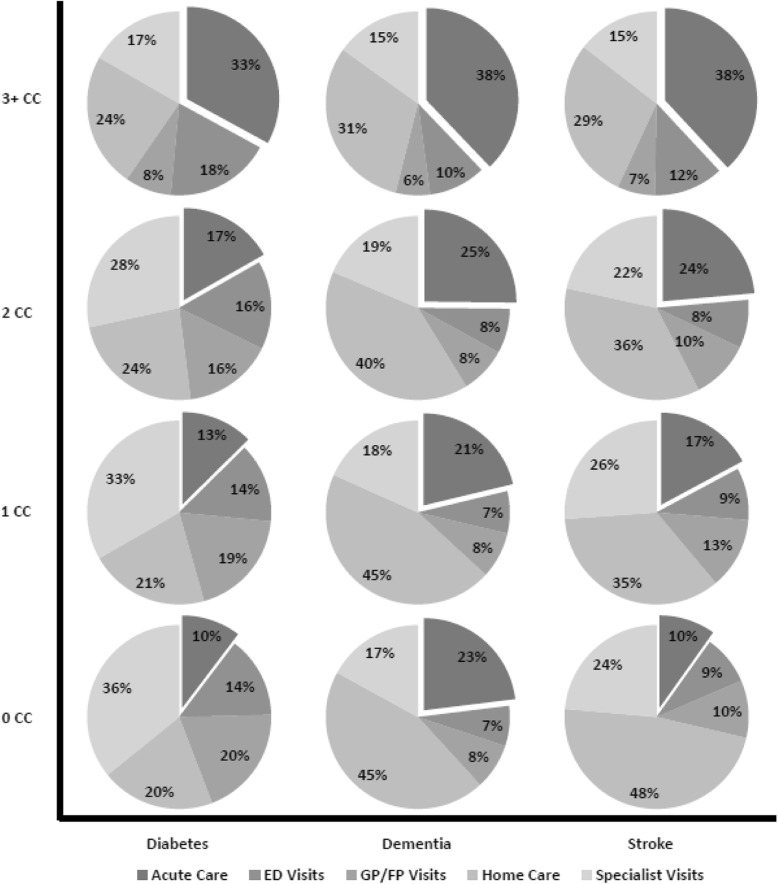
We identified 376,434 indviduals wtih diabetes, 95,399 wtih dementia, and 29,671 with stroke. Four broad insights were identified from considering the similarity in comorbidity, utilization and cost patterns across the three cohorts: 1) the most prevalent comorbidity types were hypertension and arthritis, which accounted for over 75% of comorbidity in each cohort; 2) overall utilization increased consistently with the number of comorbidities, with the vast majority of services attributed to comorbidity rather than the index conditions; 3) the biggest driver of costs for those with lower levels of comorbidity was community-based care, e.g., home care, GP visits, but at higher levels of comorbidity the driver was acute care services; 4) service-specific comorbidity and age patterns were consistent across the three cohorts.
Despite the differences in population demographics and prevalence of the three index conditions, there are common patterns with respect to comorbidity, utilization, and costs. These common patterns may illustrate underlying needs of people with multimorbidity that are often obscured in literature that is still single disease-focused.
大多数研究疾病共病及其对卫生服务利用的影响的研究都集中在单一的索引疾病上,并发表在特定疾病的期刊上,这限制了跨疾病/学科识别模式的机会。这些比较因使用不同的研究设计、多病种定义和数据源而变得更加复杂。本文旨在通过反映在同一卫生管辖区内、同一时期、使用相同研究设计和数据的三个不同疾病队列(糖尿病、痴呆和中风)中的平行研究中观察到的共病与卫生服务利用和成本之间的常见模式,分享关于多病种的见解。
我们根据三个不同疾病队列之间观察到的共病与卫生服务利用和成本之间的关系,展示了有助于更广泛了解多病种的发现。这些队列最初是使用多个链接的行政数据库创建的,以确定加拿大安大略省 2008 年患有糖尿病、痴呆或中风的社区居民,并对每个队列进行了卫生服务利用和相关成本的随访。
我们确定了 376434 名患有糖尿病的个体、95399 名患有痴呆症的个体和 29671 名患有中风的个体。从考虑三个队列中相似的共病、利用和成本模式中,我们确定了四个广泛的见解:1)最常见的共病类型是高血压和关节炎,这两种疾病占每个队列共病的 75%以上;2)随着共病数量的增加,整体利用率持续增加,绝大多数服务归因于共病而不是索引疾病;3)对于共病程度较低的患者,成本的最大驱动因素是社区为基础的护理,如家庭护理、全科医生就诊,但在共病程度较高时,驱动因素是急性护理服务;4)三个队列中特定于服务的共病和年龄模式是一致的。
尽管三个索引疾病的人群人口统计学和患病率存在差异,但在共病、利用和成本方面存在共同的模式。这些共同的模式可能说明了多病症患者的潜在需求,而这些需求在仍然以单一疾病为重点的文献中往往被掩盖。