Griffith Lauren E, Gruneir Andrea, Fisher Kathryn, Panjwani Dilzayn, Gandhi Sima, Sheng Li, Gafni Amiram, Patterson Christopher, Markle-Reid Maureen, Ploeg Jenny
Department of Clinical Epidemiology and Biostatistics, McMaster University, McMaster Innovation Park, 175 Longwood Road South, Hamilton, ON, L8P 0A1, Canada.
Department of Family Medicine, 6-40 University of Alberta, 6-10 University Terrace, Edmonton, AB, T6G 2T4, Canada.
BMC Geriatr. 2016 Oct 26;16(1):177. doi: 10.1186/s12877-016-0351-x.
Patients with dementia have increased healthcare utilization and often have comorbid chronic conditions. It is not clear if the increase in utilization is driven by dementia, the comorbidities or both. The objective of this study was to describe the number and types of comorbid conditions in a population-based cohort of older adults with dementia and how the level of comorbidity impacts dementia-related and non-dementia-related health service utilization.
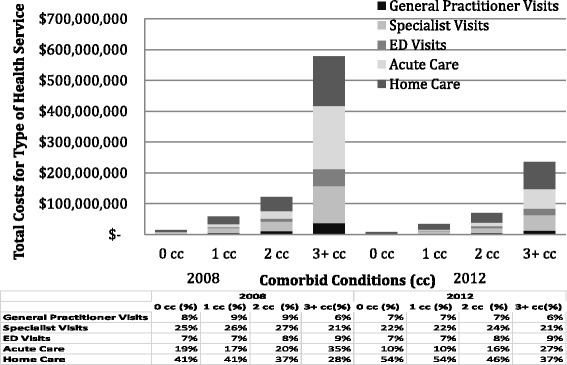
This study is a retrospective cohort study using multiple linked administrative databases to examine health service utilization and costs of 100,630 community-living older adults living with pre-existing dementia in Ontario, Canada. Comorbid conditions and health service utilization were measured using administrative data (physician visits, emergency department visits, hospitalizations, and homecare contacts).
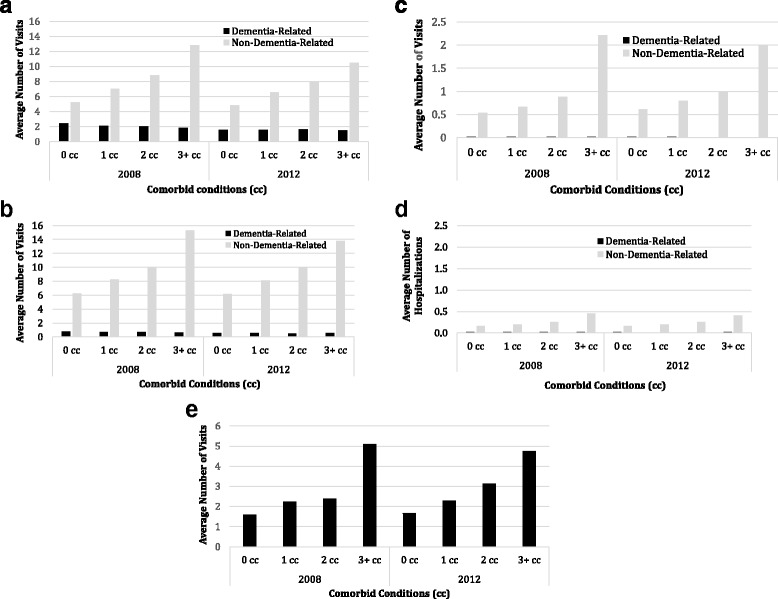
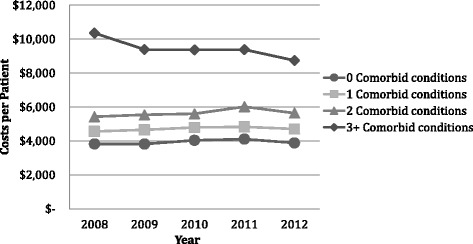
Nearly all, 96.3 %, had at least one comorbid condition, while 18.4 % had five or more comorbid conditions. The most common comorbid conditions were hypertension (77.8 %), and arthritis (66.2 %). All types of utilization increased consistently with the number of comorbid conditions. The average number of dementia-related services tended to be similar across all levels of comorbidity while the average number of non-dementia related visits tended to increase with the level of comorbidity.
Comorbidities in community-living older adults with dementia are common and account for a substantial proportion of health service use and costs in this population. Our results suggest that comprehensive programs that take a holistic view to identify the needs of patients in the context of other comorbidities are required for persons with dementia living in the community.
痴呆症患者的医疗保健利用率增加,且常常患有合并慢性病。目前尚不清楚利用率的增加是由痴呆症、合并症还是两者共同驱动的。本研究的目的是描述以社区为基础的老年痴呆症患者队列中合并症的数量和类型,以及合并症的程度如何影响与痴呆症相关和非痴呆症相关的医疗服务利用情况。
本研究是一项回顾性队列研究,使用多个相互关联的行政数据库来检查加拿大安大略省100,630名患有痴呆症的社区居住老年人的医疗服务利用情况和费用。使用行政数据(医生就诊、急诊就诊、住院和家庭护理接触)来衡量合并症和医疗服务利用情况。
几乎所有患者(96.3%)至少有一种合并症,而18.4%的患者有五种或更多合并症。最常见的合并症是高血压(77.8%)和关节炎(66.2%)。所有类型的利用率都随着合并症数量的增加而持续增加。在所有合并症水平上,与痴呆症相关服务的平均数量往往相似,而非痴呆症相关就诊的平均数量往往随着合并症程度的增加而增加。
社区居住的老年痴呆症患者合并症很常见,并且在该人群的医疗服务使用和费用中占很大比例。我们的结果表明,对于居住在社区中的痴呆症患者,需要有全面的项目,从整体角度来识别患者在其他合并症背景下的需求。