Terayama Takero, Tanaka Yoshihiro, Soga Shigeyoshi, Tsujimoto Hironori, Yoshimura Yuya, Sekine Yasumasa, Akitomi Shinji, Ikeuchi Hisashi
Department of Traumatology and Critical Care Medicine, National Defense Medical College Hospital, Namiki 3-2, Tokorozawa, Saitama, 359-8513, Japan.
Department of Radiology, National Defense Medical College Hospital, Namiki 3-2, Tokorozawa, Saitama, 359-8513, Japan.
BMC Surg. 2019 May 17;19(1):50. doi: 10.1186/s12893-019-0514-8.
A pancreaticoduodenal artery aneurysm (PDAA) occurring in close association with median arcuate ligament syndrome (MALS) is rare. A surgical procedure, such as median arcuate ligament (MAL) release, should be considered in such cases, but the operative criteria remain unknown. In this study, we reported an extremely rare case of PDAA with periarteritis nodosa (PAN) and MALS.
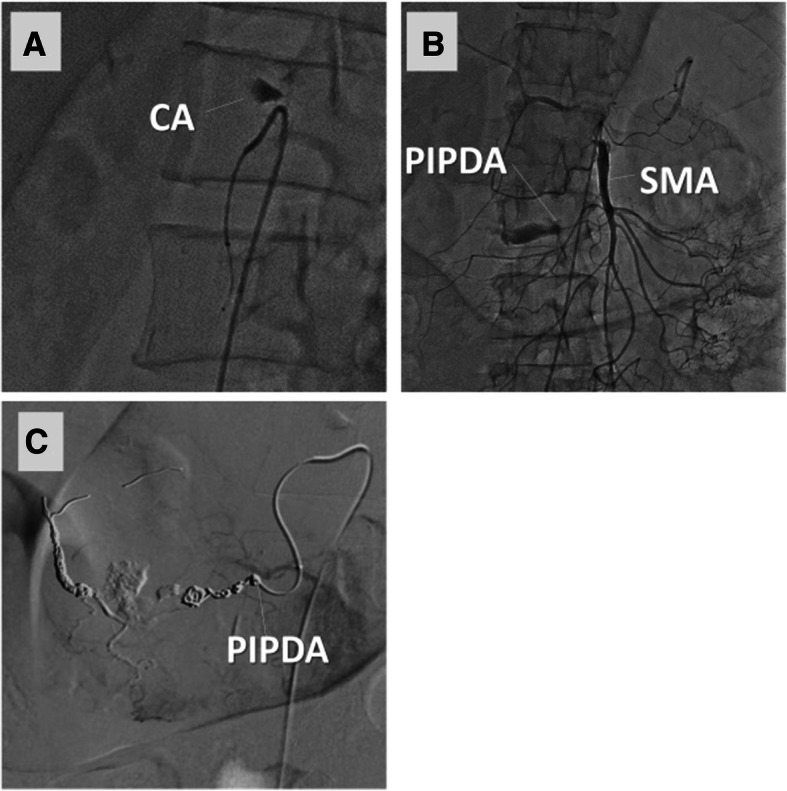
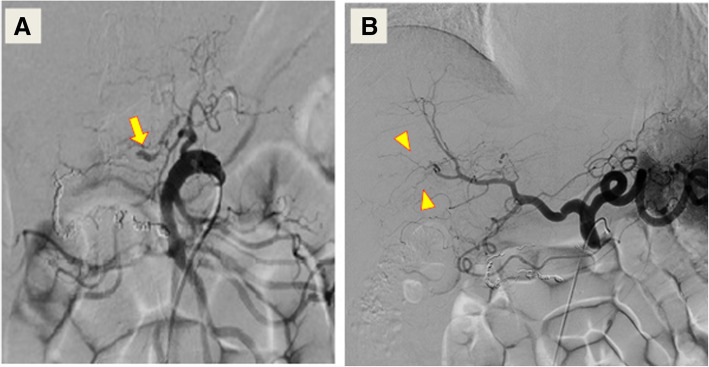
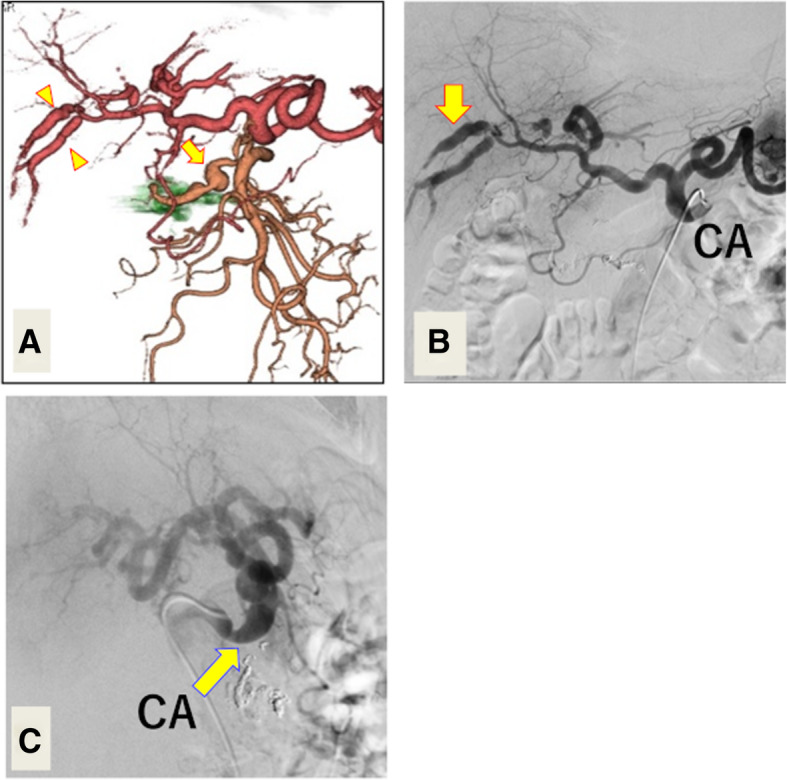
A 60-year-old man was transferred to our department with sudden onset of abdominal pain. We initially diagnosed his condition as a PDAA rupture with MALS based on enhanced computed tomography (CT). We promptly performed transcatheter arterial embolization (TAE) of PDAA, and the angiogram showed stagnant contrast agent in the celiac trunk, indicating total celiac artery occlusion. Follow-up enhanced CT three weeks after the first TAE clearly demonstrated newly formed, multiple aneurysms in the pancreaticoduodenal arcade and the hepatic artery. These findings indicated a systemic disorder, such as PAN or segmental arterial mediolysis, as the underlying cause. Therefore, we started corticosteroid therapy and performed diagnostic angiography to clarify the celiac artery's patency. Contrary to the initial angiography, the second angiography showed sustained blood flow in the celiac artery. Nevertheless, we performed both extrinsic MAL release and consecutive TAE because of the risk of multiple aneurysms rupturing due to an uncontrolled systemic disorder and consequent hepatic ischemia. The patient had no episode of recurrence until one year of follow-up.
It is important to evaluate risk for hemodynamically unstable events to decide the best treatment strategy for MALS.
与正中弓状韧带综合征(MALS)密切相关的胰十二指肠动脉瘤(PDAA)较为罕见。在此类病例中应考虑采取手术治疗,如正中弓状韧带(MAL)松解术,但手术标准仍不明确。在本研究中,我们报告了一例极为罕见的合并结节性多动脉炎(PAN)和MALS的PDAA病例。
一名60岁男性因突发腹痛被转至我科。基于增强计算机断层扫描(CT),我们最初将其病情诊断为合并MALS的PDAA破裂。我们迅速对PDAA进行了经导管动脉栓塞术(TAE),血管造影显示腹腔干内造影剂滞留,提示腹腔干完全闭塞。首次TAE三周后的随访增强CT清楚地显示在胰十二指肠动脉弓和肝动脉中有新形成的多个动脉瘤。这些发现表明潜在病因是一种全身性疾病,如PAN或节段性动脉中层溶解。因此,我们开始使用皮质类固醇治疗,并进行诊断性血管造影以明确腹腔干的通畅情况。与最初的血管造影结果相反,第二次血管造影显示腹腔干血流持续存在。尽管如此,由于全身性疾病失控导致多个动脉瘤破裂以及随之而来的肝缺血风险,我们还是进行了外在MAL松解术和连续TAE。在长达一年的随访期内,患者未出现复发情况。
评估血流动力学不稳定事件的风险对于确定MALS的最佳治疗策略很重要。