Williams Steven E, O'Neill Louisa, Roney Caroline H, Julia Justo, Metzner Andreas, Reißmann Bruno, Mukherjee Rahul K, Sim Iain, Whitaker John, Wright Matthew, Niederer Steven, Sohns Christian, O'Neill Mark
Division of Imaging Sciences and Biomedical Engineering, King's College London, London, United Kingdom.
Department of Cardiology, Asklepios Klinik St. Georg, Hamburg, Germany.
J Cardiovasc Electrophysiol. 2019 Sep;30(9):1416-1427. doi: 10.1111/jce.13990. Epub 2019 Jun 18.
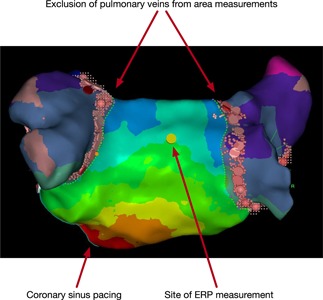
The multiple wavelets and functional re-entry hypotheses are mechanistic theories to explain atrial fibrillation (AF). If valid, a chamber's ability to support AF should depend upon the left atrial size, conduction velocity (CV), and refractoriness. Measurement of these parameters could provide a new therapeutic target for AF. We investigated the relationship between left atrial effective conducting size (LA ), a function of area, CV and refractoriness, and AF vulnerability in patients undergoing AF ablation.
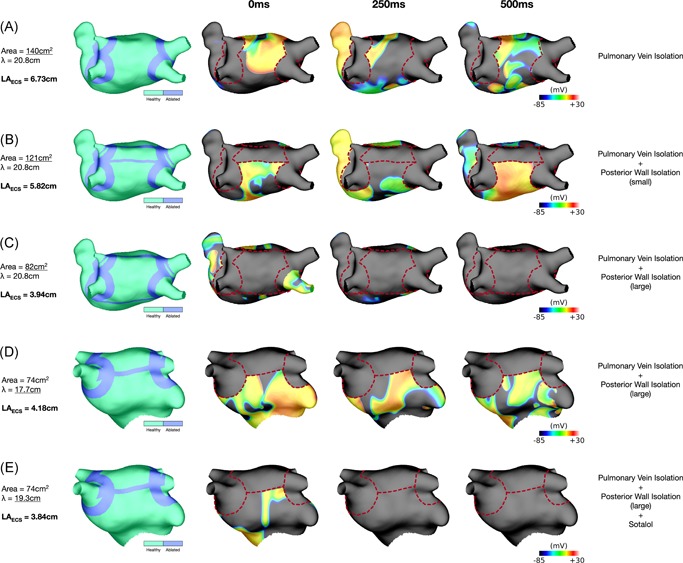
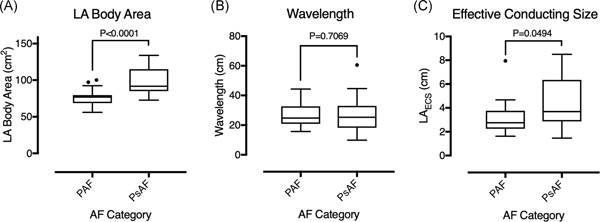
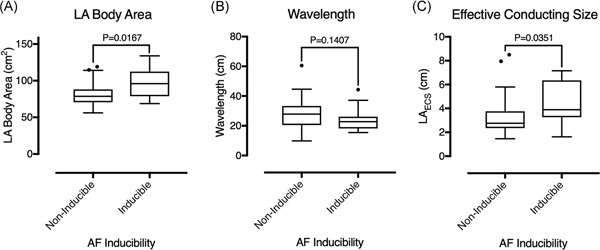
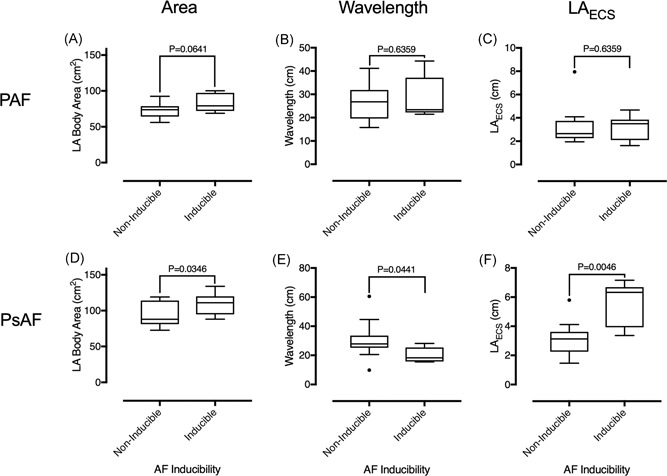
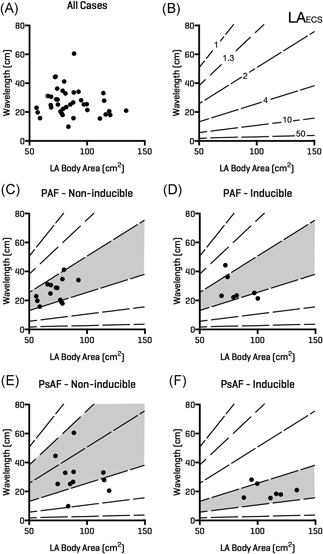
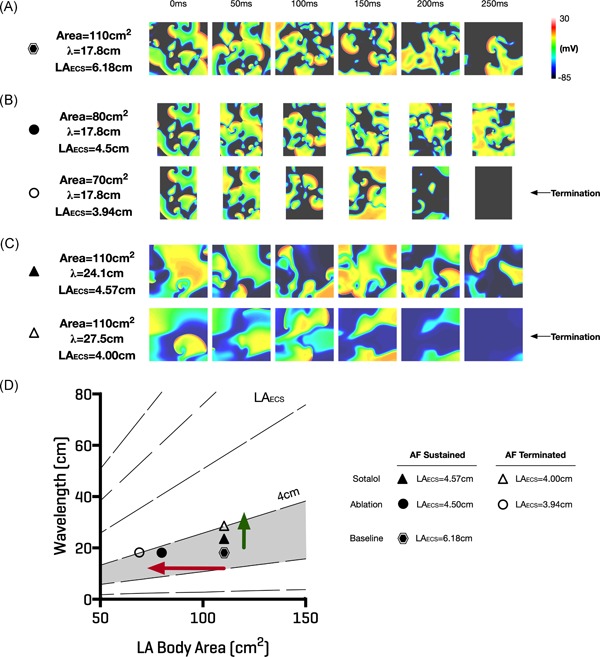
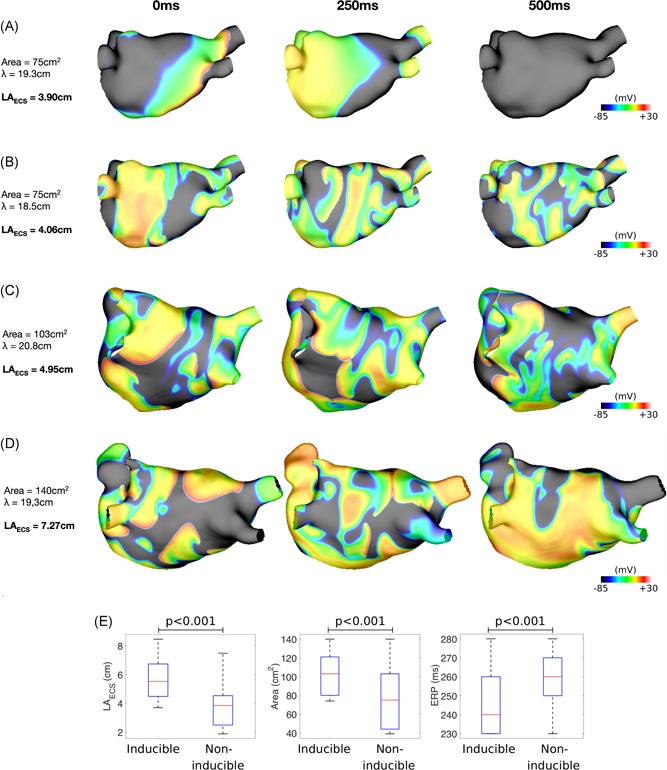
Activation mapping was performed in patients with paroxysmal (n = 21) and persistent AF (n = 18) undergoing pulmonary vein isolation. Parameters used for calculating LA were: (a) left atrial body area (A); (b) effective refractory period (ERP); and (c) total activation time (T). Global CV was estimated as . Effective atrial conducting size was calculated as . Post ablation, AF inducibility testing was performed. The critical LA required for multiple wavelet termination was determined from computational modeling. LA was greater in patients with persistent vs paroxysmal AF (4.4 ± 2.0 cm vs 3.2 ± 1.4 cm; P = .049). AF was inducible in 14/39 patients. LA was greater in AF-inducible patients (4.4 ± 1.8 cm vs 3.3 ± 1.7 cm; P = .035, respectively). The difference in LA between inducible and noninducible patients was significant in patients with persistent (P = .0046) but not paroxysmal AF (P = .6359). Computational modeling confirmed that LA > 4 cm was required for continuation of AF.
LA measured post ablation was associated with AF inducibility in patients with persistent, but not paroxysmal AF. These data support a role for this method in electrical substrate assessment in AF patients.
多小波和功能性折返假说是解释心房颤动(AF)的机制理论。如果成立,一个腔室支持房颤的能力应取决于左心房大小、传导速度(CV)和不应期。这些参数的测量可为房颤提供新的治疗靶点。我们研究了左心房有效传导面积(LA)(面积、CV和不应期的函数)与接受房颤消融患者房颤易感性之间的关系。
对21例阵发性房颤和18例持续性房颤患者进行肺静脉隔离时进行激动标测。用于计算LA的参数为:(a)左心房体面积(A);(b)有效不应期(ERP);(c)总激动时间(T)。整体CV估计为 。有效心房传导面积计算为 。消融后,进行房颤诱发试验。通过计算模型确定多小波终止所需的临界LA。持续性房颤患者的LA大于阵发性房颤患者(4.4±2.0 cm对3.2±1.4 cm;P = 0.049)。39例患者中有14例可诱发房颤。可诱发房颤患者的LA更大(分别为4.4±1.8 cm对3.3±1.7 cm;P = 0.035)。持续性房颤患者(P = 0.0046)可诱发和不可诱发患者之间的LA差异显著,但阵发性房颤患者(P = 0.6359)无显著差异。计算模型证实房颤持续需要LA>4 cm。
消融后测量的LA与持续性房颤而非阵发性房颤患者的房颤诱发有关。这些数据支持该方法在房颤患者电基质评估中的作用。