Department of Public Health and Community Medicine/Primary Health Care (J.R., M.A.), Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Sweden.
Sahlgrenska University Hospital, Gothenburg, Sweden (J.R., M.S., M.L., A.R.).
Circulation. 2019 Jul 9;140(2):117-125. doi: 10.1161/CIRCULATIONAHA.118.039132. Epub 2019 May 28.
Modifiable lifestyle factors in relation to risk for cardiomyopathy, a common and increasing cause of heart failure in the young, have not been widely studied. We sought to investigate a potential link between obesity, a recognized predictor of early heart failure, in adolescence and being diagnosed with cardiomyopathy in adulthood.
This was a nationwide register-based prospective cohort study of 1 668 893 adolescent men (mean age, 18.3 years; SD, 0.7 years) who enlisted for compulsory military service from 1969 to 2005. At baseline, body mass index (BMI), blood pressure, and medical disorders were registered, along with test results for fitness and muscle strength. Cardiomyopathy diagnoses were identified from the National Hospital Register and Cause of Death Register during an up to 46-year follow-up and divided into categories: dilated, hypertrophic, alcohol/drug-induced, and other. Hazard ratios were calculated with Cox proportional hazards models.
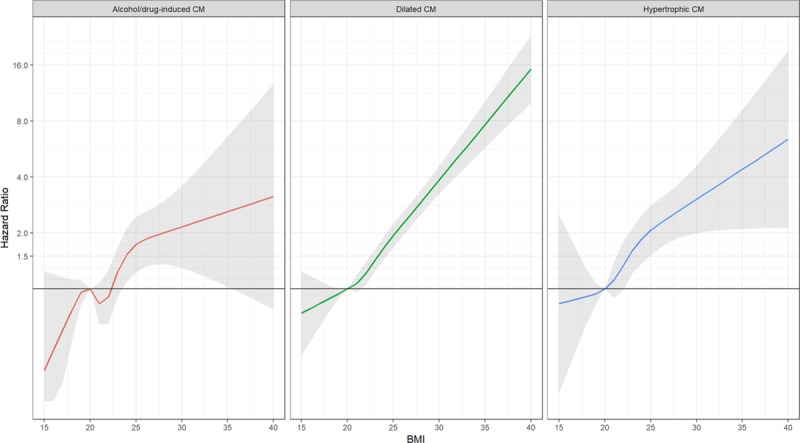
During follow-up (median, 27 years; Q1-Q3, 19-35 years), 4477 cases of cardiomyopathy were identified, of which 2631 (59%) were dilated, 673 (15%) were hypertrophic, and 480 (11%) were alcohol/drug-induced. Increasing BMI was strongly associated with elevated risk of cardiomyopathy, especially dilated, starting at levels considered normal (BMI, 22.5-<25 kg/m; hazard ratio, 1.38 [95% CI, 1.22-1.57]), adjusted for age, year, center, and baseline comorbidities, and with a >8-fold increased risk at BMI ≥35 kg/m compared with BMI of 18.5 to <20 kg/m. For each 1-unit increase in BMI, similarly adjusted hazard ratios were 1.15 (95% CI, 1.14-1.17) for dilated cardiomyopathy, 1.09 (95% CI, 1.06-1.12) for hypertrophic cardiomyopathy, and 1.10 (1.06-1.13) for alcohol/drug-induced cardiomyopathy.
Even mildly elevated body weight in late adolescence may contribute to being diagnosed with cardiomyopathy in adulthood. The already marked importance of weight control in youth is further strengthened by these findings, as well as greater evidence for obesity as a potential important cause of adverse cardiac remodeling that is independent of clinically evident ischemic heart disease.
与心肌病风险相关的可改变的生活方式因素是年轻人中常见且日益增加的心力衰竭原因,但尚未得到广泛研究。我们试图研究肥胖症(早期心力衰竭的公认预测因素)与成年后被诊断为心肌病之间的潜在联系。
这是一项全国范围内基于登记的前瞻性队列研究,纳入了 1668893 名 18.3 岁(标准差,0.7 岁)的青春期男性,他们于 1969 年至 2005 年应征入伍。在基线时,记录了体重指数(BMI)、血压和医疗疾病,以及体能和肌肉力量的测试结果。通过国家医院登记处和死因登记处,在长达 46 年的随访期间确定心肌病的诊断,并分为扩张型、肥厚型、酒精/药物诱导型和其他类型。使用 Cox 比例风险模型计算风险比。
在随访期间(中位数,27 年;Q1-Q3,19-35 年),共发现 4477 例心肌病,其中 2631 例(59%)为扩张型,673 例(15%)为肥厚型,480 例(11%)为酒精/药物诱导型。BMI 的增加与心肌病风险的升高密切相关,尤其是扩张型,从被认为正常的水平(BMI,22.5-<25 kg/m;风险比,1.38 [95% CI,1.22-1.57])开始,调整年龄、年份、中心和基线合并症后,与 BMI≥35 kg/m 相比,BMI 为 18.5 至<20 kg/m 的风险增加超过 8 倍。对于 BMI 每增加 1 个单位,同样调整后的风险比分别为扩张型心肌病 1.15(95% CI,1.14-1.17)、肥厚型心肌病 1.09(95% CI,1.06-1.12)和酒精/药物诱导型心肌病 1.10(1.06-1.13)。
即使在青春期后期体重略有升高,也可能导致成年后被诊断为心肌病。这些发现以及更多关于肥胖作为潜在重要的导致不良心脏重构的原因的证据,进一步强化了青年时期控制体重的重要性,肥胖症独立于临床明显的缺血性心脏病也是导致不良心脏重构的一个潜在重要原因。