Department of Surgical, Oncological and Oral Science (Di.Chir.On.S.). Section of Anesthesia, Analgesia, Intensive Care and Emergency, Policlinico Paolo Giaccone, University of Palermo, via del vespro 129, 90127, Palermo, Italy.
Infectious Diseases Division, Department of Medicine, University of Udine and Santa Maria della Misericordia University Hospital, Piazzale Santa Maria della Misericordia 15, Udine, Italy.
Crit Care. 2019 May 28;23(1):190. doi: 10.1186/s13054-019-2481-y.
Procalcitonin (PCT) is a biomarker used to assess systemic inflammation, infection, and sepsis and to optimize antimicrobial therapies. Its role in the in the differential diagnosis between candidemia and bacteremia is unclear. The aim of this systematic review was to summarize the current evidence about PCT values for differentiating candidemia from bacteremia.
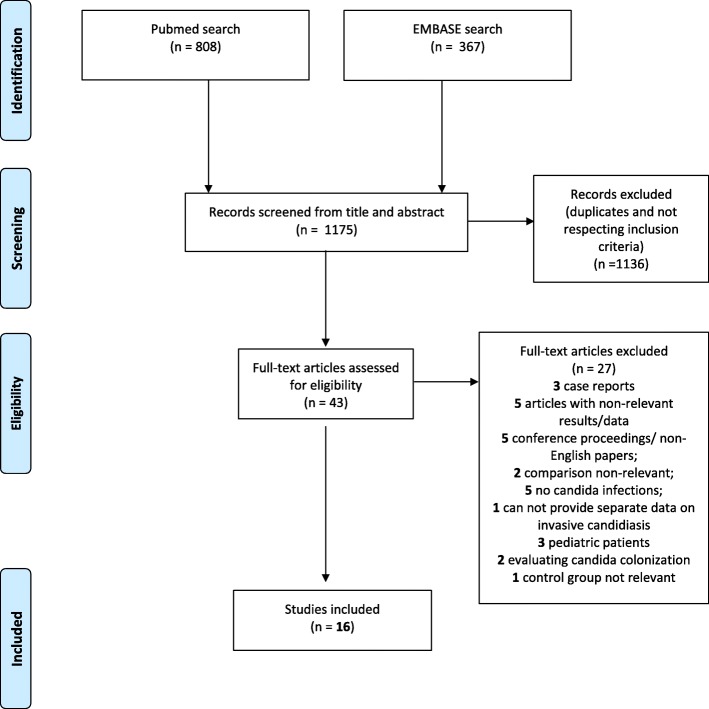
PubMed and EMBASE were searched for studies reporting data on the diagnostic performance of serum PCT levels in intensive care unit (ICU) or non-ICU adult patients with candidemia, in comparison to patients with bacteremia.
We included 16 studies for a total of 45.079 patients and 785 cases of candidemia. Most studies claimed to report data relating to the use of PCT values for differentiating between candidemia and bacteremia in septic patients in the intensive care unit. However, the studies identified were all retrospective, except for one secondary analysis of a prospective dataset, and clinically very heterogeneous and involved different assessment methods. Most studies did show lower PCT values in patients with candidemia compared to bacteremia. However, the evidence supporting this observation is of low quality and the difference seems insufficiently discriminative to guide therapeutic decisions. None of the studies retrieved actually studied guidance of antifungal treatment by PCT. PCT may improve diagnostic performance regarding candidemia when combined with other biomarkers of infection (e.g., beta-D-glucan) but more data is needed.
PCT should not be used as a standalone tool for the differential diagnosis between candidemia and bacteremia due to limited supporting evidence.
降钙素原(PCT)是一种用于评估全身炎症、感染和败血症的生物标志物,可优化抗菌治疗。其在鉴别念珠菌血症和菌血症方面的作用尚不清楚。本系统评价的目的是总结目前关于 PCT 值鉴别念珠菌血症和菌血症的证据。
检索 PubMed 和 EMBASE 数据库,以获取关于 ICU 或非 ICU 成年患者念珠菌血症和菌血症的血清 PCT 水平诊断性能的研究数据。
共纳入 16 项研究,总计 45079 例患者和 785 例念珠菌血症病例。大多数研究声称报告了与 PCT 值用于鉴别 ICU 败血症患者的念珠菌血症和菌血症相关的数据。然而,除了一项前瞻性数据集的二次分析外,所有研究均为回顾性研究,且临床差异较大,涉及不同的评估方法。大多数研究确实表明念珠菌血症患者的 PCT 值低于菌血症患者。然而,支持这一观察结果的证据质量较低,差异似乎不足以指导治疗决策。检索到的研究实际上并未研究 PCT 对指导抗真菌治疗的作用。当与其他感染标志物(如β-D-葡聚糖)联合使用时,PCT 可能会提高对念珠菌血症的诊断性能,但需要更多的数据。
由于支持证据有限,PCT 不应作为鉴别念珠菌血症和菌血症的单独工具使用。