Department of Radiation Oncology and Image-Applied Therapy, Graduate School of Medicine, Kyoto University, 54 Shogoin Kawahara-cho, Sakyo-ku, Kyoto, 606-8507, Japan.
Department of Urology, Graduate School of Medicine, Kyoto University, 54 Shogoin Kawahara-cho, Sakyo-ku, Kyoto, 606-8507, Japan.
Int J Clin Oncol. 2019 Oct;24(10):1247-1255. doi: 10.1007/s10147-019-01478-y. Epub 2019 May 31.
The optimal timing of salvage androgen deprivation therapy (ADT) following definitive radiation therapy for prostate cancer (PCa) is unknown. This study evaluated the efficacy of early initiation of salvage-ADT (S-ADT) based on predetermined timing among patients with unfavorable PCa treated with high-dose intensity-modulated radiation therapy (IMRT).
High-risk (HR) and very-high-risk (VHR) PCa patients treated with IMRT at our institution between September 2000 and December 2010 were analyzed retrospectively. Treatment consisted of high-dose IMRT (78 Gy/39 fractions) combined with 6 months of neoadjuvant-ADT (NA-ADT). S-ADT was initiated when prostate-specific antigen levels exceeded 4.0 ng/mL.
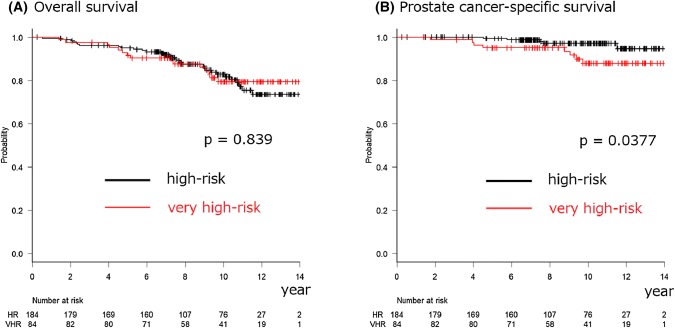
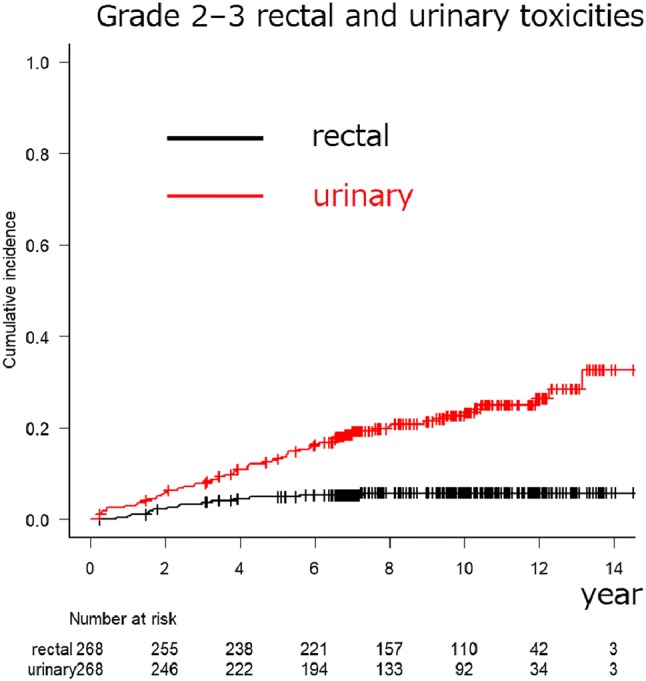
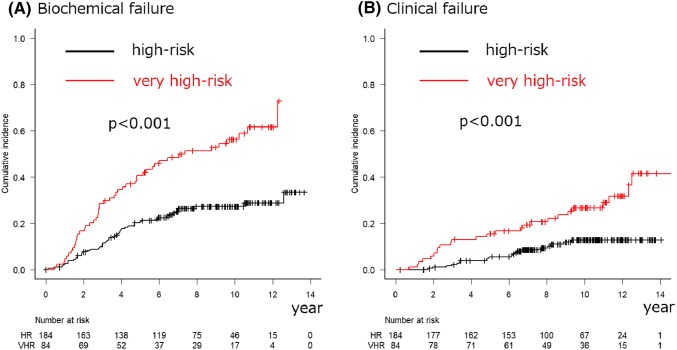
In total, 268 (184 HR and 84 VHR) patients were analyzed. The median follow-up period was 114.4 months. The 10-year overall survival (OS), PCa-specific survival (PCSS), biochemical failure (BF), and clinical failure (CF) rates were 82.8%, 97.1%, 27.3%, and 12.8% among the HR PCa patients and 79.4%, 87.9%, 56.2%, and 26.7% among the VHR PCa patients (p = 0.839, = 0.0377, < 0.001, and < 0.001), respectively. The 10-year cumulative incidence rates of urinary and rectal (grades 2-3) toxicities were 22.6% and 5.8%, respectively. No grade 4 or higher toxicities were observed.
High-dose IMRT combined with short-term NA-ADT resulted in long-term disease-free status, with acceptable morbidity among approximately three-fourths of the HR PCa patients and nearly half of the VHR PCa patients. Moreover, excellent survival outcomes were achieved by the early S-ADT initiation. This approach may be a promising alternative to uniform provision of long-term ADT.
根治性放疗后挽救性雄激素剥夺治疗(ADT)的最佳时机尚不清楚。本研究评估了在我院接受高剂量强度调制放疗(IMRT)治疗的高危(HR)和极高危(VHR)前列腺癌(PCa)患者中,根据预设时间提前开始挽救性 ADT(S-ADT)的疗效。
回顾性分析了我院于 2000 年 9 月至 2010 年 12 月期间接受 IMRT 治疗的高危和极高危 PCa 患者。治疗包括高剂量 IMRT(78 Gy/39 次)联合 6 个月的新辅助 ADT(NA-ADT)。当前列腺特异性抗原(PSA)水平超过 4.0ng/ml 时开始 S-ADT。
共分析了 268 例(184 例 HR 和 84 例 VHR)患者。中位随访时间为 114.4 个月。HR PCa 患者的 10 年总生存率(OS)、前列腺癌特异性生存率(PCSS)、生化失败(BF)和临床失败(CF)率分别为 82.8%、97.1%、27.3%和 12.8%,VHR PCa 患者分别为 79.4%、87.9%、56.2%和 26.7%(p=0.839,=0.0377,<0.001,<0.001)。10 年累积尿和直肠(2-3 级)毒性发生率分别为 22.6%和 5.8%。未观察到 4 级或更高毒性。
高剂量 IMRT 联合短期 NA-ADT 可实现长期无疾病状态,约四分之三的 HR PCa 患者和近一半的 VHR PCa 患者的发病率可接受。此外,早期开始 S-ADT 可获得良好的生存结果。这种方法可能是一种有前途的替代方案,以替代长期 ADT 的统一提供。