Division of Vascular and Endovascular Surgery, University of California, San Francisco, Calif.
Department of Vascular Surgery, University of Birmingham, Birmingham, United Kingdom.
J Vasc Surg. 2019 Jun;69(6S):3S-125S.e40. doi: 10.1016/j.jvs.2019.02.016. Epub 2019 May 28.
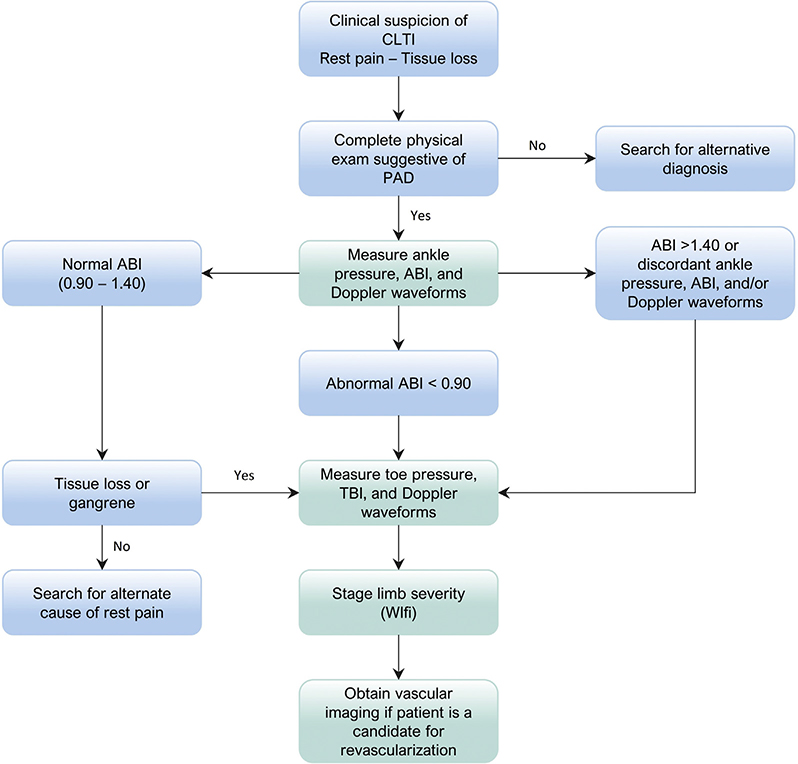
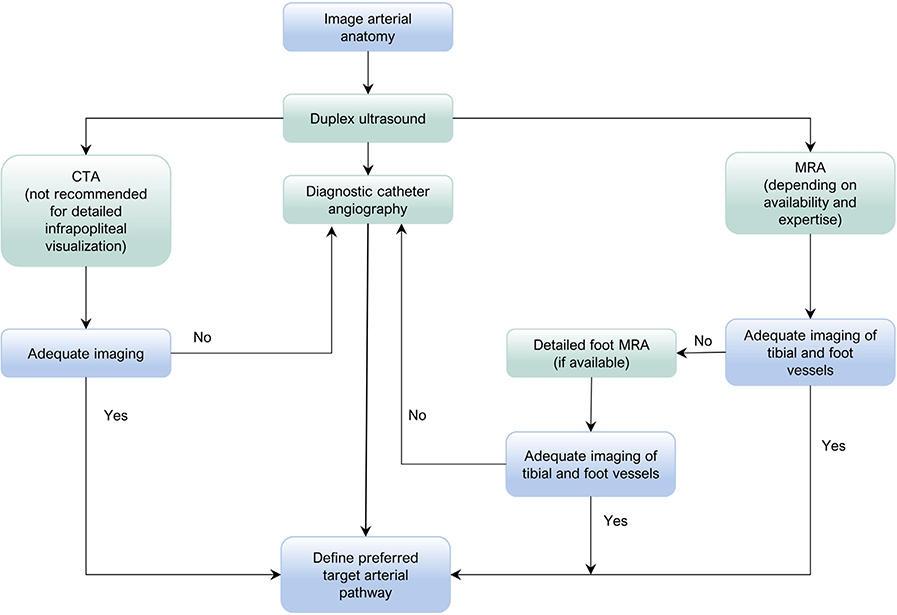
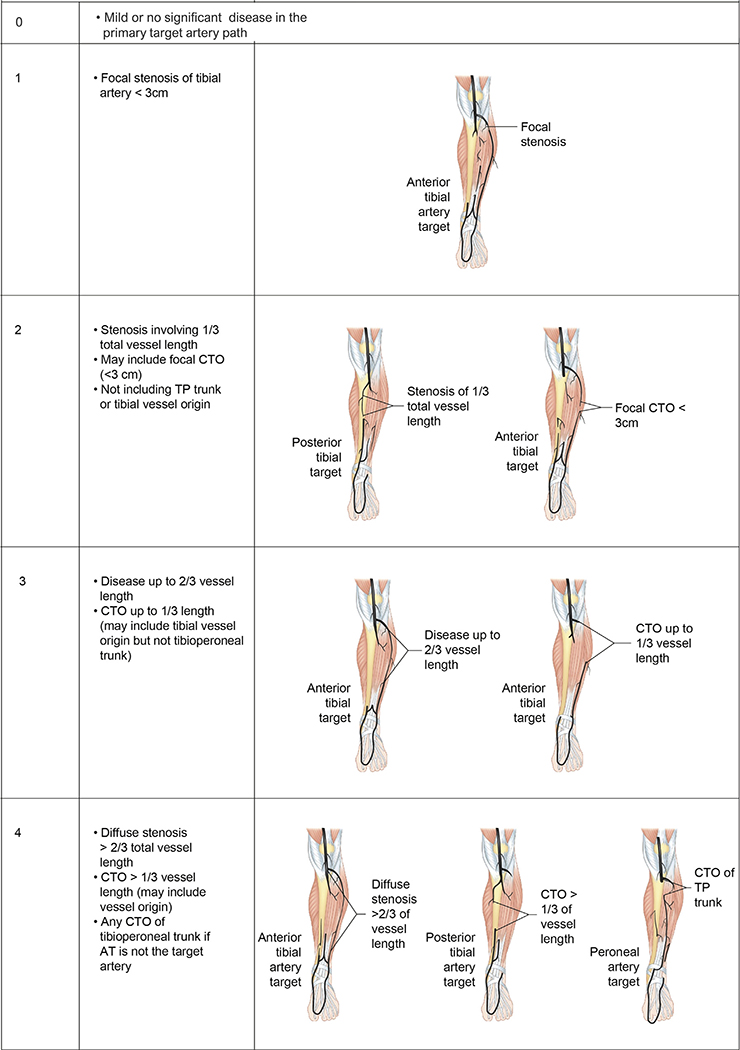
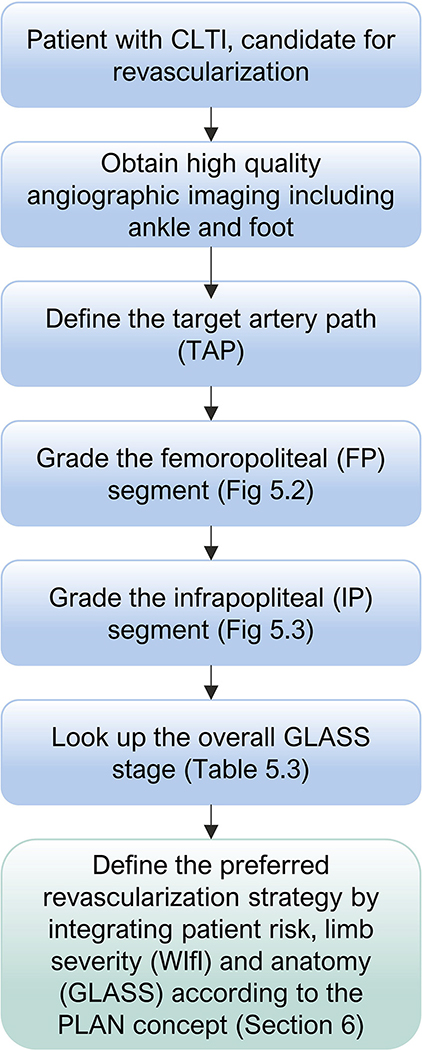
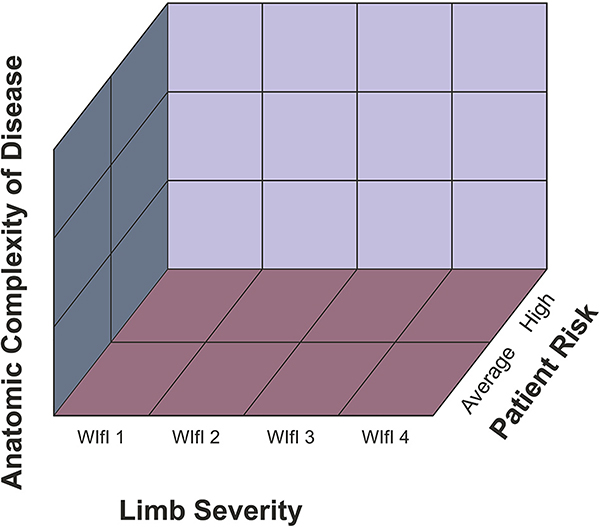
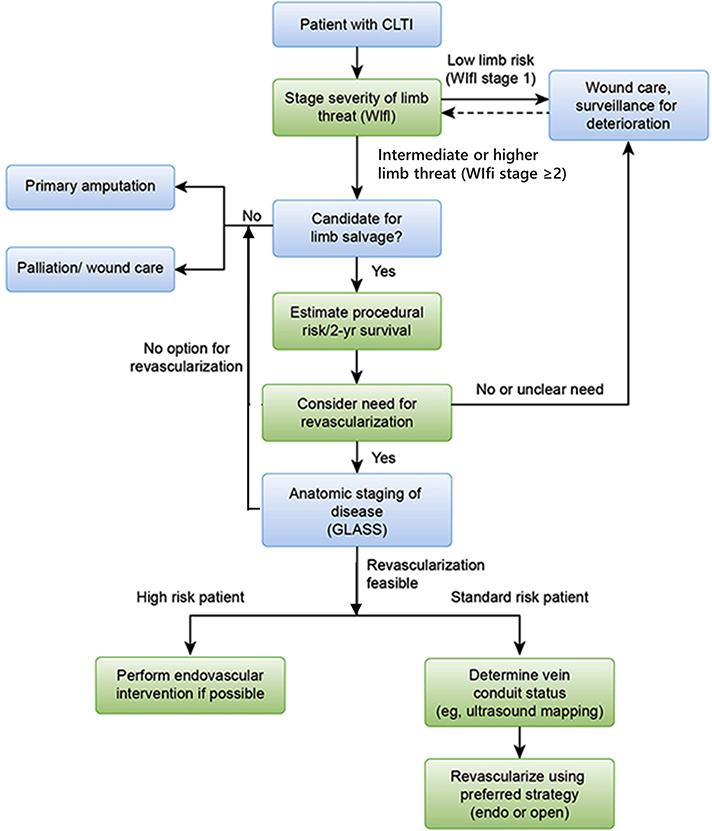
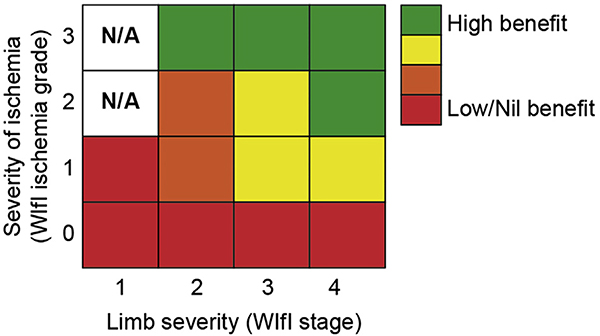
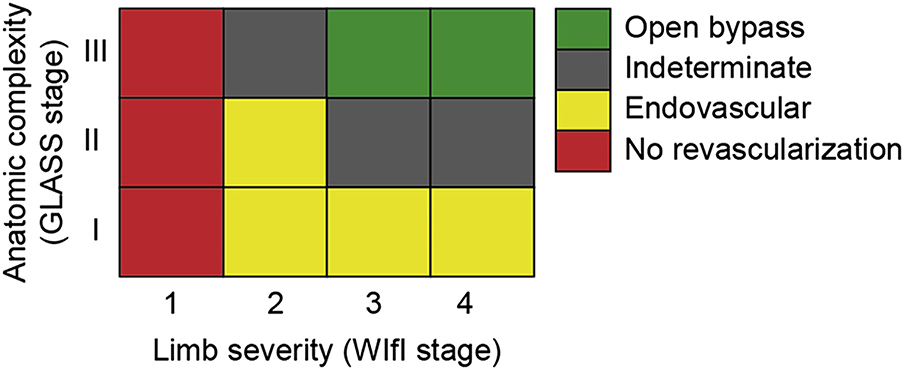
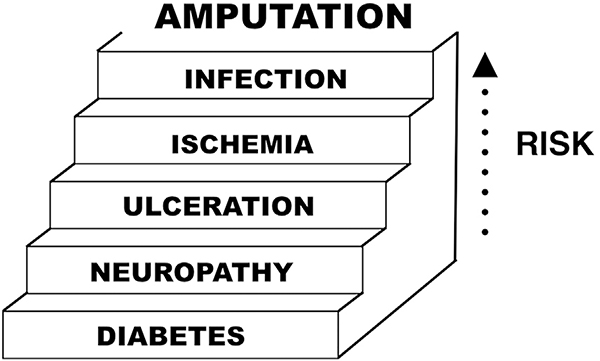
Chronic limb-threatening ischemia (CLTI) is associated with mortality, amputation, and impaired quality of life. These Global Vascular Guidelines (GVG) are focused on definition, evaluation, and management of CLTI with the goals of improving evidence-based care and highlighting critical research needs. The term CLTI is preferred over critical limb ischemia, as the latter implies threshold values of impaired perfusion rather than a continuum. CLTI is a clinical syndrome defined by the presence of peripheral artery disease (PAD) in combination with rest pain, gangrene, or a lower limb ulceration >2 weeks duration. Venous, traumatic, embolic, and nonatherosclerotic etiologies are excluded. All patients with suspected CLTI should be referred urgently to a vascular specialist. Accurately staging the severity of limb threat is fundamental, and the Society for Vascular Surgery Threatened Limb Classification system, based on grading of Wounds, Ischemia, and foot Infection (WIfI) is endorsed. Objective hemodynamic testing, including toe pressures as the preferred measure, is required to assess CLTI. Evidence-based revascularization (EBR) hinges on three independent axes: Patient risk, Limb severity, and ANatomic complexity (PLAN). Average-risk and high-risk patients are defined by estimated procedural and 2-year all-cause mortality. The GVG proposes a new Global Anatomic Staging System (GLASS), which involves defining a preferred target artery path (TAP) and then estimating limb-based patency (LBP), resulting in three stages of complexity for intervention. The optimal revascularization strategy is also influenced by the availability of autogenous vein for open bypass surgery. Recommendations for EBR are based on best available data, pending level 1 evidence from ongoing trials. Vein bypass may be preferred for average-risk patients with advanced limb threat and high complexity disease, while those with less complex anatomy, intermediate severity limb threat, or high patient risk may be favored for endovascular intervention. All patients with CLTI should be afforded best medical therapy including the use of antithrombotic, lipid-lowering, antihypertensive, and glycemic control agents, as well as counseling on smoking cessation, diet, exercise, and preventive foot care. Following EBR, long-term limb surveillance is advised. The effectiveness of nonrevascularization therapies (eg, spinal stimulation, pneumatic compression, prostanoids, and hyperbaric oxygen) has not been established. Regenerative medicine approaches (eg, cell, gene therapies) for CLTI should be restricted to rigorously conducted randomizsed clinical trials. The GVG promotes standardization of study designs and end points for clinical trials in CLTI. The importance of multidisciplinary teams and centers of excellence for amputation prevention is stressed as a key health system initiative.
慢性肢体严重缺血(CLTI)与死亡率、截肢和生活质量受损有关。这些全球血管指南(GVG)专注于 CLTI 的定义、评估和管理,旨在改善循证护理并突出关键研究需求。术语 CLTI 优于严重肢体缺血,因为后者意味着灌注受损的阈值值,而不是连续体。CLTI 是一种临床综合征,定义为存在外周动脉疾病(PAD),同时伴有静息痛、坏疽或下肢溃疡 >2 周。排除静脉、创伤性、栓塞性和非动脉粥样硬化病因。所有疑似 CLTI 的患者均应紧急转介至血管专科医生。准确分期肢体威胁的严重程度至关重要,基于伤口、缺血和足部感染(WIfI)分级的血管外科学会威胁肢体分类系统得到认可。客观的血流动力学测试,包括首选的趾压测试,是评估 CLTI 所必需的。循证血运重建(EBR)取决于三个独立的轴:患者风险、肢体严重程度和解剖复杂性(PLAN)。平均风险和高风险患者是根据估计的手术和 2 年全因死亡率来定义的。GVG 提出了一种新的全球解剖分期系统(GLASS),它涉及定义首选的靶动脉路径(TAP),然后估计基于肢体的通畅率(LBP),从而导致干预的三个复杂阶段。最佳血运重建策略也受到用于开放旁路手术的自体静脉可用性的影响。EBR 的建议基于最佳可用数据,等待正在进行的试验提供 1 级证据。对于严重肢体威胁和高复杂性疾病的平均风险患者,静脉旁路可能更受欢迎,而对于解剖结构较简单、中等严重程度肢体威胁或高患者风险的患者,血管内介入可能更有利。所有 CLTI 患者均应接受最佳药物治疗,包括使用抗血栓、降脂、降压和血糖控制药物,以及戒烟、饮食、运动和预防性足部护理咨询。EBR 后,建议长期进行肢体监测。非血运重建治疗(例如,脊髓刺激、气动压缩、前列腺素和高压氧)的有效性尚未确定。CLTI 的再生医学方法(例如,细胞、基因治疗)应仅限于严格进行的随机临床试验。GVG 促进了 CLTI 临床试验的研究设计和终点的标准化。强调多学科团队和卓越中心在预防截肢方面的重要性,这是一项关键的卫生系统倡议。