University of Rochester, Rochester, New York.
University of Virginia, Charlottesville, Virginia.
Epilepsia. 2019 Jul;60(7):1453-1461. doi: 10.1111/epi.16072. Epub 2019 Jun 11.
To determine whether a less-invasive approach to surgery for medically refractory temporal lobe epilepsy is associated with lower health care costs and costs of lost productivity over time, compared to open surgery.
We compared direct medical costs and indirect productivity costs associated with treatment with stereotactic radiosurgery (SRS) or anterior temporal lobectomy (ATL) in the ROSE (Radiosurgery or Open Surgery for Epilepsy) trial. Health care use was abstracted from hospital bills, the study database, and diaries in which participants recorded health care use and time lost from work while seeking care. Costs of use were calculated using a Medicare costing approach used in a prior study of the costs of ATL. The power of many analyses was limited by the sample size and data skewing.
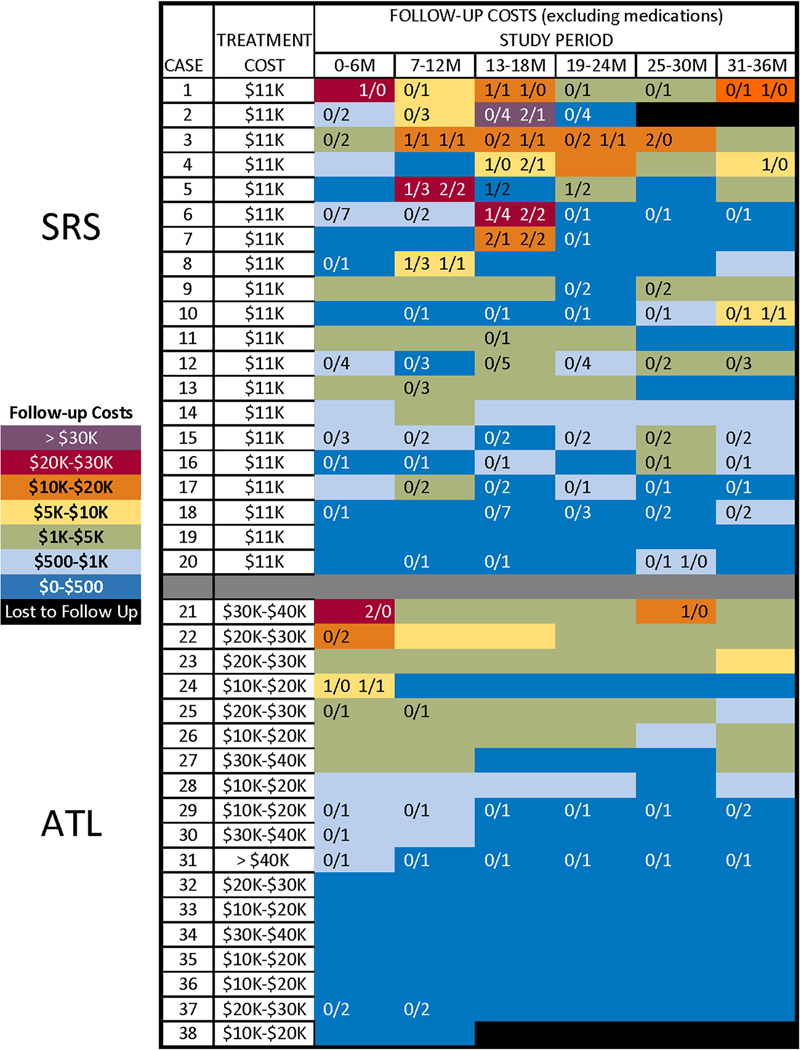
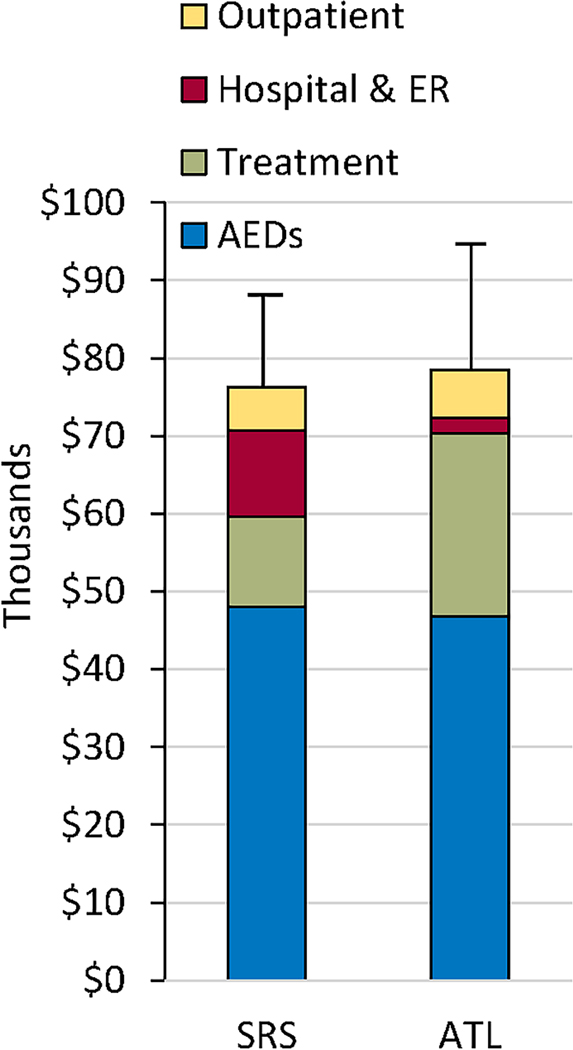
Combined treatment and follow-up costs (in thousands of US dollars) did not differ between SRS (n = 20, mean = $76.6, 95% confidence interval [CI] = 50.7-115.6) and ATL (n = 18, mean = $79.0, 95% CI = 60.09-103.8). Indirect costs also did not differ. More ATL than SRS participants were free of consciousness-impairing seizures in each year of follow-up (all P < 0.05). Costs declined following ATL (P = 0.005). Costs tended to increase over the first 18 months following SRS (P = 0.17) and declined thereafter (P = 0.06). This mostly reflected hospitalizations for SRS-related adverse events in the second year of follow-up.
Lower initial costs of SRS for medial temporal lobe epilepsy were largely offset by hospitalization costs related to adverse events later in the course of follow-up. Future studies of less-invasive alternatives to ATL will need to assess adverse events and major costs systematically and prospectively to understand the economic implications of adopting these technologies.
与开颅手术相比,确定对于药物难治性颞叶癫痫患者,采用侵袭性较小的手术方法是否会降低医疗成本和长期生产力损失成本。
我们比较了 ROSE(癫痫的放射外科手术或开颅手术)试验中立体定向放射外科手术(SRS)或前颞叶切除术(ATL)治疗的直接医疗成本和间接生产力损失成本。从医院账单、研究数据库以及参与者记录求医过程中医疗保健使用情况和工作时间损失的日记中提取医疗保健使用情况。使用先前 ATL 成本研究中使用的 Medicare 成本计算方法计算使用成本。由于样本量和数据偏斜,许多分析的效力受到限制。
SRS(n=20,平均值=76.6,95%置信区间[CI] = 50.7-115.6)和 ATL(n=18,平均值=79.0,95%CI = 60.09-103.8)的联合治疗和随访费用(以千美元计)之间没有差异。间接成本也没有差异。在随访的每一年,ATL 参与者无意识障碍性癫痫发作的比例均高于 SRS 参与者(均 P<0.05)。ATL 后成本下降(P=0.005)。SRS 后成本在随访的头 18 个月内呈上升趋势(P=0.17),此后呈下降趋势(P=0.06)。这主要反映了在随访第二年与 SRS 相关的不良事件导致的住院治疗。
SRS 治疗内侧颞叶癫痫的初始成本较低,但在随访过程中因不良事件而导致的住院费用在很大程度上抵消了这一优势。未来对 ATL 替代方案的研究需要系统地、前瞻性地评估不良事件和主要成本,以了解采用这些技术的经济影响。