Huang Chen, Shi Qingyi, Zheng Beiwen, Ji Jinru, Ying Chaoqun, Yu Xiao, Wang Hui, Xiao Yonghong
State Key Laboratory for Diagnosis and Treatment of Infectious Disease, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People's Republic of China.
Department of Respiratory Medicine, Lihuili Hospital, Ningbo Medical Center, Ningbo, People's Republic of China.
Infect Drug Resist. 2019 May 8;12:1199-1208. doi: 10.2147/IDR.S193712. eCollection 2019.
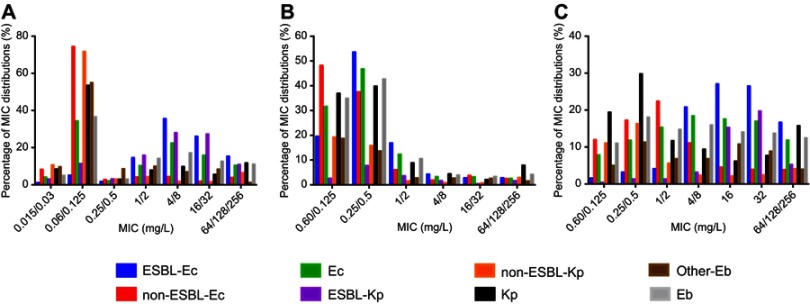
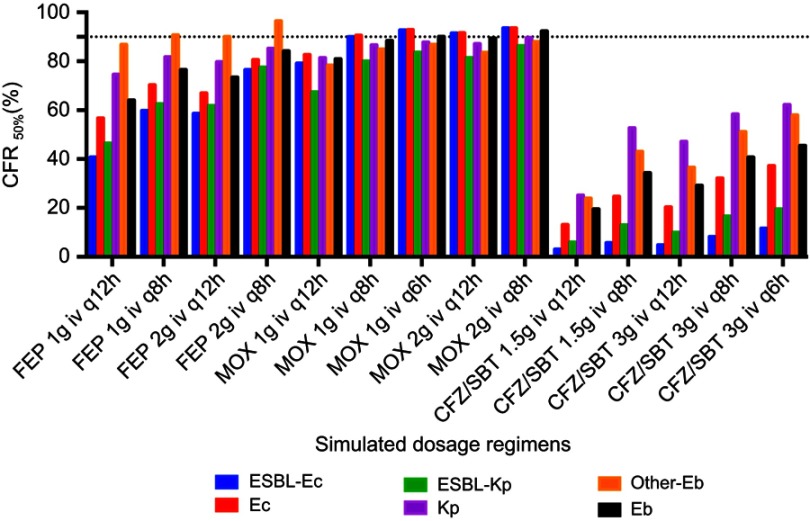
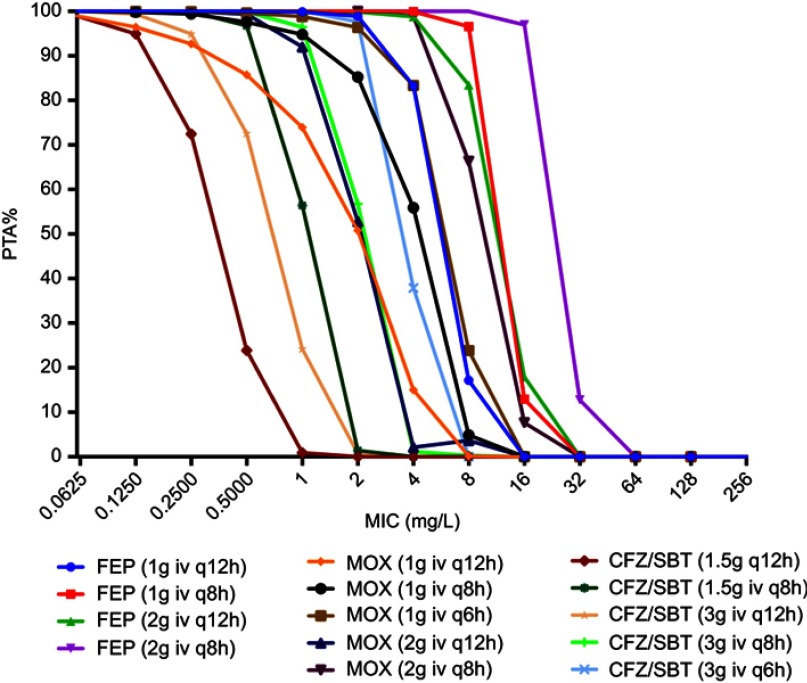
Monte Carlo simulation (MCS) was used to evaluate optimal dosage for cefepime (FEP), moxalactam (MOX), and cefperazone/sulbactam (CFZ/SBT) against extended-spectrum β-lactamase (ESBL) producers isolated from the Blood Bacterial Resistant Investigation Collaborative System. : Minimum inhibitory concentration (MIC) was tested by agar dilution, and ESBL producers were identified by modified Clinical and Laboratory Standards Institute tests. Pharmacokinetic parameters were derived from data on healthy individuals, and probability of target attainment (PTA) and cumulative fraction of response (CFR) %fT >MIC values were estimated by MCS. A total of 2032 (875 ESBL-producing) and (157 ESBL-producing) strains, and 371 other strains, were isolated from patients with bloodstream infections (BSIs). MIC values for FEP, MOX, and CFZ/SBT against ESBL-producing and were 64/64 mg/L, 2/32 mg/L, and 64/128 mg/L, respectively. Conventional MOX and CFZ/SBT doses failed to reach 90% PTA against isolates with MICs ≥8 mg/L and ≥4 mg/L, respectively. Against ESBL producers, neither FEP nor CFZ/SBT achieved ≥90% CFR, while CFRs for MOX (1 g iv q6h, 2 g iv q12h, and 2 g iv q8h) exceeded 90% against ESBL-producing . Simulated CFRs for FEP and MOX were similar (>90%) against non-ESBL-producing , and higher than CFRs for CFZ/SBT. ESBL producers from BSIs were highly susceptible to MOX, and PTA values were generally higher for MOX than FEP or CFZ/SBT for conventional dosing regimens. This large MCS analysis shows that MOX but not FEP or CFZ/SBT can be used empirically to treat BSIs caused by ESBL-producing strains.
采用蒙特卡罗模拟(MCS)评估头孢吡肟(FEP)、拉氧头孢(MOX)和头孢哌酮/舒巴坦(CFZ/SBT)对从血液细菌耐药性调查协作系统分离出的产超广谱β-内酰胺酶(ESBL)菌株的最佳剂量。通过琼脂稀释法检测最低抑菌浓度(MIC),并通过改良的临床和实验室标准协会试验鉴定产ESBL菌株。药代动力学参数来源于健康个体的数据,通过MCS估计目标达成概率(PTA)和反应累积分数(CFR)%fT>MIC值。从血流感染(BSI)患者中分离出总共2032株(875株产ESBL)和(157株产ESBL)菌株,以及371株其他菌株。FEP、MOX和CFZ/SBT对产ESBL的和的MIC值分别为64/64 mg/L、2/32 mg/L和64/128 mg/L。传统的MOX和CFZ/SBT剂量分别未能对MIC≥8 mg/L和≥4 mg/L的分离株达到90%的PTA。对于产ESBL菌株,FEP和CFZ/SBT均未达到≥90%的CFR,而MOX(1 g静脉注射q6h、2 g静脉注射q12h和2 g静脉注射q8h)对产ESBL的CFR超过90%。FEP和MOX对非产ESBL的模拟CFR相似(>90%),且高于CFZ/SBT的CFR。BSI中产ESBL菌株对MOX高度敏感,对于传统给药方案,MOX的PTA值通常高于FEP或CFZ/SBT。这项大型MCS分析表明,MOX可凭经验用于治疗由产ESBL菌株引起的BSI,而FEP或CFZ/SBT则不行。