Jeffries Erin, Falcone-Wharton Amy, Daggy Joanne, Tucker Edmonds Brownsyne
Department of OB/GYN, Indiana University School of Medicine, Indianapolis, Indiana.
Department of Biostatistics, Indiana University School of Medicine, Indianapolis, Indiana.
MDM Policy Pract. 2019 May 27;4(1):2381468319850830. doi: 10.1177/2381468319850830. eCollection 2019 Jan-Jun.
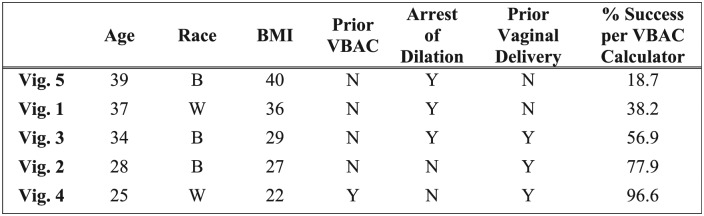
Because failed trial of labor after cesarean (TOLAC) is associated with greater morbidity than planned cesarean, it is important to distinguish women with a high likelihood of successful vaginal birth after cesarean (VBAC) from those likely to fail. The VBAC Calculator may help make this distinction but little is known about how often providers use it; nor whether use improves risk estimation and/or influences TOLAC counseling. In a cross-sectional survey, a convenience sample of obstetrical providers reported their likelihood (4-point Likert-type scale) to "Recommend,""Offer," or "Agree to" TOLAC for patients presented first through five clinical vignettes; then, in different order, by corresponding VBAC calculator estimates. Of the 85 (of 101, 84% response rate) participants, 88% routinely performed TOLAC, but only 21% used the Calculator. The majority (67.1% to 89.3%) overestimated the likelihood of success for all but one vignette (which had the highest estimate of success). Most providers (42% to 89%) recommended TOLAC for all five vignettes. Given calculated estimates, the majority of providers (67% to 95%) recommended TOLAC for success estimates exceeding 40%. For estimates between 20% and 40%, most providers offered (58%) or agreed (68%) to TOLAC; and even below 20%, over half still agreed to TOLAC. The vignette with the lowest estimate of success (18.7%) had the weakest intraprovider agreement (kappa = 0.116; confidence interval [CI] = 0.045-0.187), whereas the strongest agreement was found in the two vignettes with highest success estimates: 77.9% (kappa = 0.549; CI = 0.382-0.716) and 96.6% (kappa = 0.527; CI = 0.284-0.770). Survey responses may not reflect actual practice patterns. Providers are overly optimistic in their clinical estimation of VBAC success. Wider use of decision support could aid in risk stratification and TOLAC counseling to reduce patient morbidity.
由于剖宫产术后试产(TOLAC)失败比计划剖宫产的发病率更高,因此区分剖宫产术后阴道分娩成功可能性高的女性和可能失败的女性非常重要。VBAC计算器可能有助于做出这种区分,但对于医疗服务提供者使用它的频率知之甚少;也不清楚使用它是否能改善风险评估和/或影响TOLAC咨询。在一项横断面调查中,一个由产科医疗服务提供者组成的便利样本报告了他们对于通过五个临床病例首次呈现的患者“推荐”“提供”或“同意”TOLAC的可能性(4点李克特量表);然后,按不同顺序,根据相应的VBAC计算器估计值进行报告。在101名参与者中有85名(回复率84%),88%的人常规进行TOLAC,但只有21%的人使用了计算器。除了一个成功率估计最高的病例外,大多数人(67.1%至89.3%)高估了所有病例成功的可能性。大多数医疗服务提供者(42%至89%)对所有五个病例都推荐了TOLAC。根据计算出的估计值,大多数医疗服务提供者(67%至95%)对成功率估计超过40%的情况推荐了TOLAC。对于2