Department of Plastic Surgery, Zhongnan Hospital of Wuhan University, Wuhan, China.
Department of Pediatrics, St John Hospital and Medical Center, Detroit, MI, United States of America.
PLoS One. 2019 Jun 14;14(6):e0218171. doi: 10.1371/journal.pone.0218171. eCollection 2019.
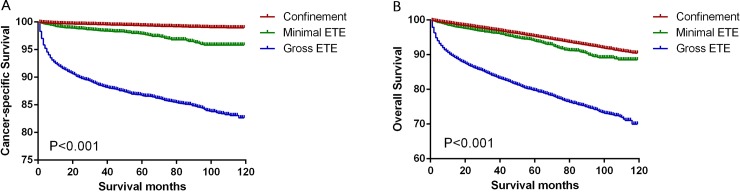
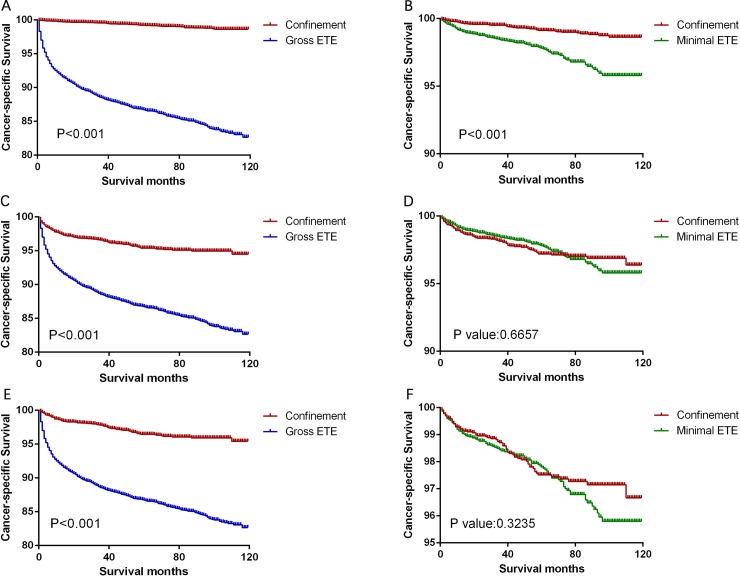
Minimal extrathyroidal extension (ETE) is defined as tumor cells extending to the sternothyroid muscle or perithyroidal soft tissue. However, there is controversy regarding whether the magnitude of ETE (minimal or gross) should be considered in assigning a precise TNM stage to patients with thyroid cancer in the seventh/eighth editions of the AJCC system. The present study evaluated Surveillance, Epidemiology, and End Results data from 107,114 patients with differentiated thyroid cancer (2004-2013) to determine whether the magnitude of ETE (thyroid confinement, minimal, or gross) influenced the ability to predict cancer-specific survival (CSS) and overall survival (OS). Patient mortality was evaluated using Cox proportional hazards regression analyses and Kaplan-Meier analyses with log-rank tests. The cancer-specific mortality rates per 1,000 person-years were 1.407 for the thyroid confinement group (95% CI: 1.288-1.536), 5.133 for the minimal ETE group (95% CI: 4.301-6.124), and 29.735 for the gross ETE group (95% CI: 28.147-31.412). Relative to the thyroid confinement group, patients with minimal ETE and gross ETE had significantly poorer CSS and OS in the univariate and multivariate analyses (both P<0.001). After propensity-score matching according to age, sex, and race, we found that thyroid confinement was associated with better CSS and OS rates than minimal ETE (P<0.001) and gross ETE (P<0.001). These results from a population-based cohort provide a reference for precise personalized treatment and management of patients with minimal ETE. Furthermore, it may be prudent to revisit the magnitude of ETE as advocated by the AJCC and currently used for treatment recommendation by the American Thyroid Association.
微小甲状腺外延伸(ETE)定义为肿瘤细胞延伸至胸骨甲状腺肌或甲状腺周围软组织。然而,在第七/八版 AJCC 系统中,对于甲状腺癌患者,是否应考虑 ETE(微小或大体)的程度来精确分配 TNM 分期仍存在争议。本研究评估了 107114 例分化型甲状腺癌(2004-2013 年)患者的监测、流行病学和最终结果数据,以确定 ETE(甲状腺限制、微小或大体)的程度是否影响预测癌症特异性生存(CSS)和总体生存(OS)的能力。使用 Cox 比例风险回归分析和 Kaplan-Meier 分析结合对数秩检验评估患者死亡率。每 1000 人年的癌症特异性死亡率分别为甲状腺限制组 1.407(95%CI:1.288-1.536)、微小 ETE 组 5.133(95%CI:4.301-6.124)和大体 ETE 组 29.735(95%CI:28.147-31.412)。与甲状腺限制组相比,微小 ETE 和大体 ETE 组在单因素和多因素分析中 CSS 和 OS 均显著较差(均 P<0.001)。根据年龄、性别和种族进行倾向评分匹配后,我们发现甲状腺限制与更好的 CSS 和 OS 率相关,优于微小 ETE(P<0.001)和大体 ETE(P<0.001)。基于人群的队列研究结果为精确的个体化治疗和管理微小 ETE 患者提供了参考。此外,重新审视 AJCC 提倡的 ETE 程度并重新审视美国甲状腺协会推荐的治疗方法可能是明智的。