Department of Obstetrics and Gynecology, Duke University Medical Center, Durham NC.
Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California-San Diego, San Diego CA.
Am J Obstet Gynecol. 2019 Sep;221(3):233.e1-233.e16. doi: 10.1016/j.ajog.2019.06.004. Epub 2019 Jun 12.
Little is known about short- and long-term pain and functional activity after surgery for pelvic organ prolapse.
The objectives of the study were to describe postoperative pain and functional activity after transvaginal native tissue reconstructive surgery with apical suspension and retropubic synthetic midurethral sling and to compare these outcomes between patients receiving 2 common transvaginal prolapse repairs, uterosacral ligament, and sacrospinous ligament vaginal vault suspension.
This planned secondary analysis of a 2 × 2 factorial randomized trial included 374 women randomized to receive uterosacral (n = 188) or sacrospinous (n = 186) vaginal vault suspension to treat both stages 2-4 apical vaginal prolapse and stress urinary incontinence between 2008 and 2013 at 9 medical centers. Participants were also randomized to receive perioperative pelvic muscle therapy or usual care. All patients received transvaginal native tissue repairs and a midurethral sling. Participants completed the Surgical Pain Scales (0-10 numeric rating scales; higher scores = greater pain) and Activity Assessment Scale (0-100; higher score = higher activity) prior to surgery and at 2 weeks, 4-6 weeks, and 3 months postoperatively. The MOS 36-item Short-Form Health Survey was completed at baseline and 6, 12, and 24 months after surgery; the bodily pain, physical functioning, and role-physical subscales were used for this analysis (higher scores = less disability). Self-reported pain medication use was also collected.
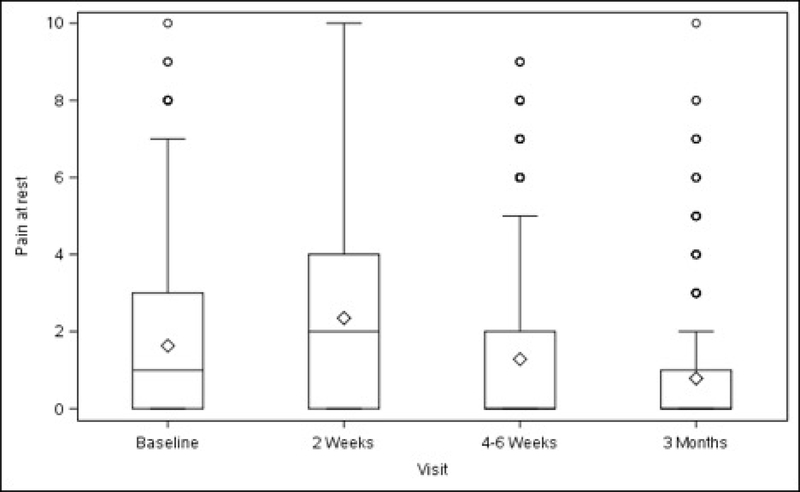
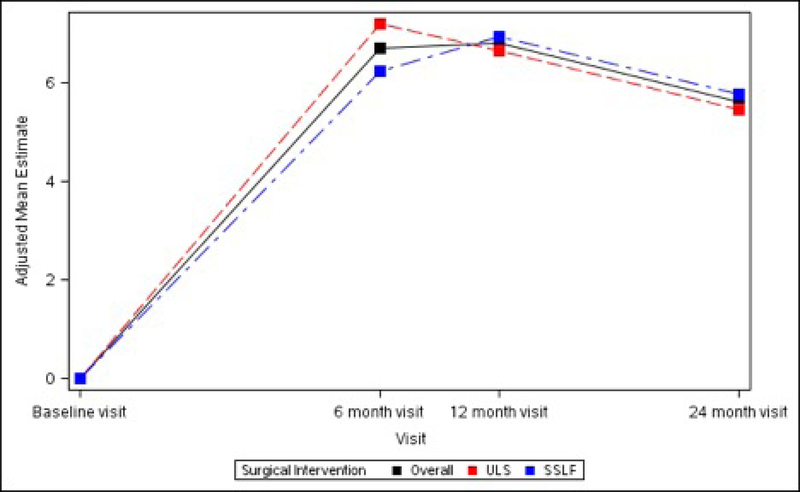
Before surgery, average pain at rest and during normal activity were (adjusted mean ± SE) 2.24 ± 0.23 and 2.76 ± 0.25; both increased slightly from baseline at 2 weeks (+0.65, P = .004, and +0.74, P = .007, respectively) and then decreased below baseline at 3 months (-0.87 and -1.14, respectively, P < .001), with no differences between surgical groups. Pain during exercise/strenuous activity and worst pain decreased below baseline levels at 4-6 weeks (-1.26, P = .014, and -0.95, P = .002) and 3 months (-1.97 and -1.50, P < .001) without differences between surgical groups. Functional activity as measured by the Activity Assessment Scale improved from baseline at 4-6 weeks (+9.24, P < .001) and 3 months (+13.79, P < .001). The MOS 36-item Short-Form Health Survey Bodily Pain, Physical Functioning, and Role-Physical Scales demonstrated significant improvements from baseline at 6, 12, and 24 months (24 months: +5.62, +5.79, and +4.72, respectively, P < .001 for each) with no differences between groups. Use of narcotic pain medications was reported by 14.3% of participants prior to surgery and 53.7% at 2 and 26.1% at 4-6 weeks postoperatively; thereafter use was similar to baseline rates until 24 months when it decreased to 6.8%. Use of nonnarcotic pain medication was reported by 48.1% of participants prior to surgery, 68.7% at 2 weeks, and similar to baseline at 3 months; thereafter use dropped steadily to 26.6% at 2 years. Uterosacral ligament suspension resulted in less new or worsening buttock pain than sacrospinous suspension at 4-6 weeks postoperatively (4.6% vs 10.5%, P = .043) but no difference in groin or thigh pain.
Pain and functional activity improve for up to 2 years after native tissue reconstructive surgery with uterosacral or sacrospinous vaginal vault suspension and midurethral sling for stages 2-4 pelvic organ prolapse. On average, immediate postoperative pain is low and improves to below baseline levels by 4-6 weeks.
对于盆腔器官脱垂患者,术后短期和长期疼痛以及功能活动情况鲜为人知。
本研究旨在描述经阴道固有组织修复术联合阴道顶端悬吊术和耻骨后合成中段尿道吊带治疗 2-4 期盆腔器官脱垂伴压力性尿失禁患者的术后疼痛和功能活动情况,并比较两种常见经阴道脱垂修复术(骶骨固定阴道穹隆悬吊术和骶棘韧带固定阴道穹隆悬吊术)的结果。
这是一项 2×2 析因随机试验的二次分析,纳入了 2008 年至 2013 年在 9 家医疗中心接受治疗的 374 名患者,她们随机接受骶骨固定阴道穹隆悬吊术(n=188)或骶棘韧带固定阴道穹隆悬吊术(n=186)治疗 2-4 期阴道顶端脱垂和压力性尿失禁,所有患者均接受经阴道固有组织修复术和中段尿道吊带。参与者还随机接受围手术期盆腔肌肉治疗或常规护理。所有患者均接受经阴道固有组织修复术和中段尿道吊带。术前及术后 2 周、4-6 周和 3 个月时,参与者使用手术疼痛量表(0-10 数字评分量表;评分越高表示疼痛越剧烈)和活动评估量表(0-100;评分越高表示活动度越高)进行评估。术前及术后 6、12 和 24 个月时,参与者使用 MOS 36 项简短健康调查问卷进行评估;本分析使用身体疼痛、身体机能和角色身体子量表(评分越高表示残疾程度越低)。还收集了自我报告的止痛药使用情况。
术前,静息时和正常活动时的平均疼痛分别为(调整后的平均±SE)2.24±0.23 和 2.76±0.25;术后 2 周时略有增加(分别增加 0.65,P=0.004 和 0.74,P=0.007),然后在 3 个月时低于基线(分别减少 0.87 和 1.14,P<0.001),两组之间无差异。运动/剧烈活动时和最剧烈疼痛时的疼痛在 4-6 周(分别减少 1.26,P=0.014 和 0.95,P=0.002)和 3 个月(分别减少 1.97 和 1.50,P<0.001)时低于基线水平,两组之间无差异。活动评估量表的功能活动从 4-6 周(增加 9.24,P<0.001)和 3 个月(增加 13.79,P<0.001)时开始改善。MOS 36 项简短健康调查问卷的身体疼痛、身体机能和角色身体量表在 6、12 和 24 个月时均显示出显著改善(24 个月时,分别增加 5.62、5.79 和 4.72,P<0.001),两组之间无差异。术前有 14.3%的参与者使用阿片类止痛药,术后 2 周时为 53.7%,4-6 周时为 26.1%;此后,止痛药的使用与基线水平相似,直到 24 个月时降至 6.8%。术前有 48.1%的参与者使用非阿片类止痛药,术后 2 周时为 68.7%,3 个月时与基线水平相似;此后,止痛药的使用持续下降,2 年后降至 26.6%。与骶棘韧带固定阴道穹隆悬吊术相比,骶骨固定阴道穹隆悬吊术在术后 4-6 周时新发或加重的臀部疼痛较少(4.6%比 10.5%,P=0.043),但在腹股沟或大腿疼痛方面无差异。
对于 2-4 期盆腔器官脱垂伴压力性尿失禁患者,行骶骨固定阴道穹隆悬吊术或骶棘韧带固定阴道穹隆悬吊术联合中段尿道吊带治疗后,疼痛和功能活动可改善长达 2 年。平均而言,术后即刻疼痛较低,在 4-6 周时可改善至低于基线水平。