Xiao Xinyu, Yu Xia, Yin Litong, Zhang Ling, Feng Dan, Zhang Lushuang, Gong Zhaolin, Zhang Qiang, Lin Yonghong, He Li
Department of Obstetrics and Gynecology, Chengdu Women's and Children's Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
Department of Clinical Laboratory, Chengdu Women's and Children's Central Hospital, Sichuan Provincial People's Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
Front Med (Lausanne). 2024 Jul 24;11:1399247. doi: 10.3389/fmed.2024.1399247. eCollection 2024.
In several randomized controlled trials (RCTs), sacrospinous hysteropexy and other forms of hysteropreservation have been compared. Nevertheless, there is no definitively best treatment. This study summarized RCT evidence for various uterine preservation surgical procedures.
From each database inception to August 2023, we searched PubMed, Embase, Cochrane Library, and Web of Science for eligible RCTs. A comparison was made between sacrospinous hysteropexy and other hysteropreservation, including vaginal and abdominal surgery. For categorical and continuous variables, relative risks (RRs) and mean differences (MDs) were calculated using random-effects models.
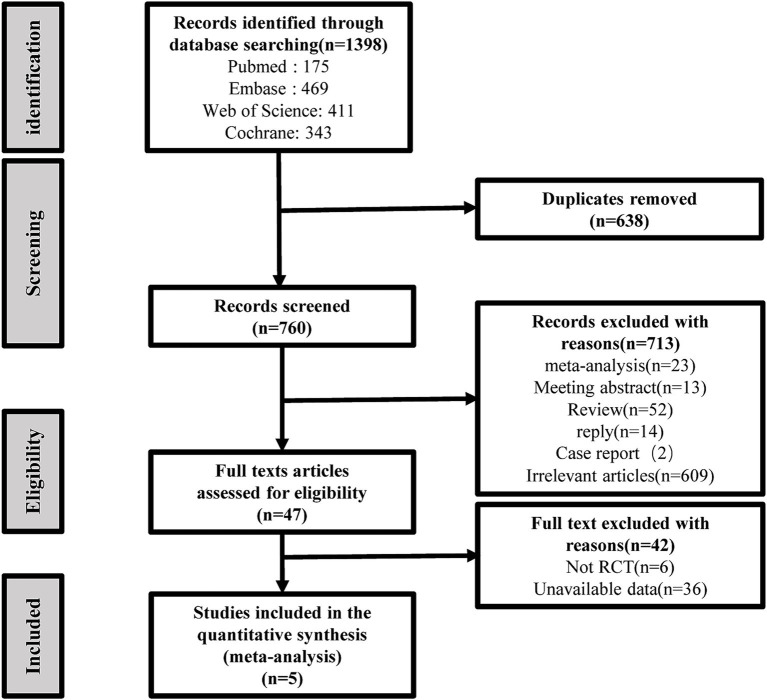
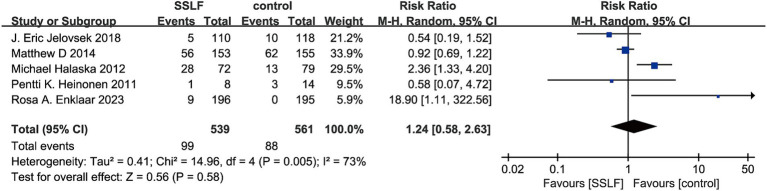
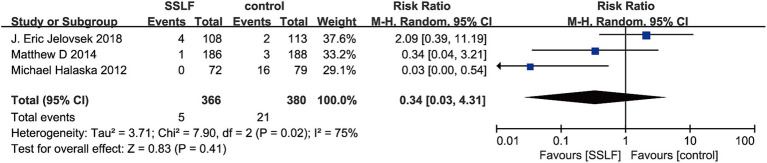
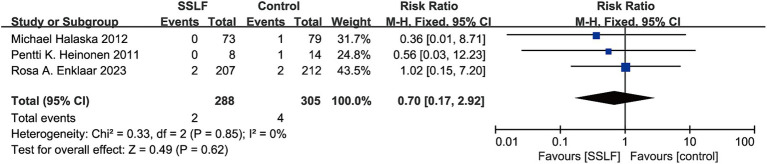
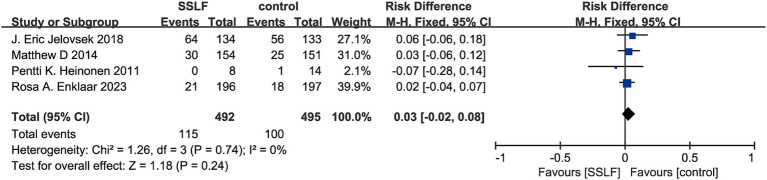
We reviewed a total 1,398 studies and ultimately included five RCTs that met all inclusion criteria. These five studies included a total of 1,372 uterine POP cases all of whom received transvaginal surgery and had a follow-up period for assessment of recurrence from 12 months to 5 years. There were no significant differences between sacrospinous hysteropexy and other hysteropreservation for the incidences of recurrence (RR,1.24; 95% CI, 0.58 to 2.63; = 0.58) or hematoma (RR,0.70; 95% CI, 0.17 to 2.92; = 0.62). Moreover, neither sacrospinous hysteropexy nor hysteropreservation had any significant effect on the risk of mesh exposure (RR,0.34; 95% CI, 0.03 to 4.31; = 0.41), dyspareunia (RR,0.45; 95% CI, 0.13 to1.6; = 0.22), urinary tract infection (RR,0.66; 95% CI, 0.38 to 1.15; = 0.15), bothersome bulge symptoms (RR,0.03; 95% CI, -0.02 to 0.08; = 0.24), operative time (MD, -4.53; 95% CI, -12.08 to 3.01; = 0.24), and blood loss (MD, -25.69; 95% CI, -62.28 to 10.91; = 0.17). However, sacrospinous hysteropexy was associated with a lower probability of pain (RR,4.8; 95% CI, 0.79 to 29.26; = 0.09) compared with other hysteropreservation.
There was no difference between sacrospinous hysteropexy and hysteropreservation in terms of recurrence, hematoma, mesh exposure, dyspareunia, urinary tract infection, bothersome bulge symptoms, operative time, pain, and blood loss.
PROSPERO [CRD42023470025].
在多项随机对照试验(RCT)中,已对骶棘韧带子宫固定术和其他形式的子宫保留术进行了比较。然而,尚无明确的最佳治疗方法。本研究总结了各种子宫保留手术的RCT证据。
从各数据库建库至2023年8月,我们在PubMed、Embase、Cochrane图书馆和科学网中检索符合条件的RCT。对骶棘韧带子宫固定术与其他子宫保留术(包括阴道手术和腹部手术)进行了比较。对于分类变量和连续变量,使用随机效应模型计算相对风险(RR)和平均差(MD)。
我们共检索了1398项研究,最终纳入了5项符合所有纳入标准的RCT。这5项研究共纳入1372例子宫脱垂病例,所有患者均接受经阴道手术,随访评估复发时间为12个月至5年。骶棘韧带子宫固定术与其他子宫保留术在复发率(RR,1.24;95%CI,0.58至2.63;P = 0.58)或血肿发生率(RR,0.70;95%CI,0.17至2.92;P = 0.62)方面无显著差异。此外,骶棘韧带子宫固定术和子宫保留术对网片暴露风险(RR,0.34;95%CI,0.03至4.31;P = 0.41)、性交困难(RR,0.45;95%CI,0.13至1.6;P = 0.22)、尿路感染(RR,0.66;95%CI,0.38至1.15;P = 0.15)、烦人的膨出症状(RR,0.03;95%CI,-0.02至0.08;P = 0.24)、手术时间(MD,-4.53;95%CI,-12.08至3.01;P = 0.24)和失血量(MD,-25.69;95%CI,-62.28至10.91;P = 0.17)均无显著影响。然而,与其他子宫保留术相比,骶棘韧带子宫固定术疼痛发生率较低(RR,4.8;95%CI,0.79至29.26;P = 0.09)。
骶棘韧带子宫固定术与子宫保留术在复发、血肿、网片暴露、性交困难、尿路感染、烦人的膨出症状、手术时间、疼痛和失血量方面无差异。
PROSPERO [CRD42023470025]