Krentz Hartmut B, Vu Quang, Gill M John
Southern Alberta Clinic, Calgary, Canada.
Department of Medicine, University of Calgary, Calgary, Canada.
Open Forum Infect Dis. 2019 Apr 26;6(6):ofz203. doi: 10.1093/ofid/ofz203. eCollection 2019 Jun.
Cross-sectional reporting of viral suppression rates within a population underestimates the community viral load (VL) burden. Longitudinal approaches, while addressing cumulative effects, may still underestimate viral burden if "churn" (movement in and out of care) is not incorporated. We examined the impact of churn on the cumulative community HIV viral burden.
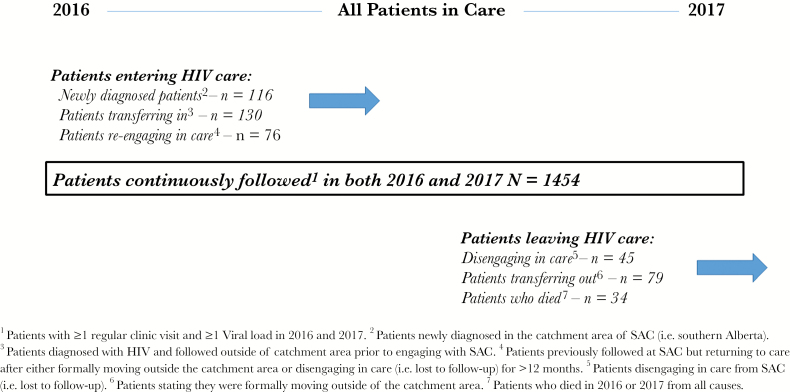
All HIV+ patients followed in 2016-2017 at the Southern Alberta Clinic (Calgary, Canada) were categorized as follows: (1) in continuous care, (2) newly diagnosed, (3) diagnosed elsewhere transferring care, (4) returning to care, (5) lost-to-follow-up, (6) moved care elsewhere, or (7) died. Patient days were classified by VL as suppressed (≤200copies/ml), unsuppressed (>200 copies/ml), and transmittable (>1500 copies/ml).
Of 1934 patients, 78.4% had suppressed VL; 21.4% had ≥1 unsuppressed VL, and 18.7% ≥1 transmittable VL. Of 1 276 507 total patient days in care, 92.1% were spent suppressed, 7.9% unsuppressed (101 459 days), and 6.4% (81 847 days) transmittable. 88.7% of category 1 patients had suppressed VL, 11.3% ≥1 unsuppressed VL, and 8.9% ever a transmittable VL. Of category 2 patients, 90% became suppressed on treatment (mean - 62 days). 38.5% of category 3 patients presented with a transmittable VL. Category 4 and 5 patients combined had high rates of unsuppressed (54.5%) and transmittable (51.2%) VL and, while representing only 6.2% of all patients, they accounted for 37.1% of unsuppressed and 41.5% of all transmittable days.
Focus on VL of patients continuously in care misses those with unsuppressed and transmittable VL in a community. Patients moving in and out of care pose an underappreciated risk for HIV transmissions.
对人群中病毒抑制率进行横断面报告低估了社区病毒载量(VL)负担。纵向研究方法虽然能解决累积效应问题,但如果未纳入“人员变动”(接受治疗和停止治疗的情况),仍可能低估病毒负担。我们研究了人员变动对社区累积HIV病毒负担的影响。
2016 - 2017年在加拿大卡尔加里南艾伯塔诊所接受随访的所有HIV阳性患者分为以下几类:(1)持续接受治疗;(2)新诊断;(3)在其他地方诊断后转来接受治疗;(4)恢复治疗;(5)失访;(6)转至其他地方接受治疗;或(7)死亡。按病毒载量将患者天数分类为病毒被抑制(≤200拷贝/毫升)、未被抑制(>200拷贝/毫升)和具有传染性(>1500拷贝/毫升)。
1934例患者中,78.4%的患者病毒载量被抑制;21.4%的患者有≥1次未被抑制的病毒载量,18.7%的患者有≥1次具有传染性的病毒载量。在接受治疗的1276507个患者天数中,92.1%的时间病毒载量被抑制,7.9%未被抑制(101459天),6.4%(81847天)具有传染性。第1类患者中88.7%的病毒载量被抑制,11.3%有≥1次未被抑制的病毒载量,8.9%曾有具有传染性的病毒载量。第2类患者中,90%在治疗后病毒载量被抑制(平均 - 62天)。第3类患者中38.5%的病毒载量具有传染性。第4类和第5类患者合并后,未被抑制(54.5%)和具有传染性(51.2%)的病毒载量发生率很高,虽然仅占所有患者的6.2%,但却占未被抑制天数的37.1%和所有具有传染性天数的41.5%。
关注持续接受治疗患者的病毒载量会遗漏社区中病毒载量未被抑制和具有传染性的患者。接受治疗和停止治疗的患者对HIV传播构成了未被充分认识的风险。