Can J Kidney Health Dis. 2019 Jun 10;6:2054358119852937. doi: 10.1177/2054358119852937. eCollection 2019.
The optimal timing of renal replacement therapy (RRT) initiation in critically ill patients with acute kidney injury (AKI) remains controversial.
In critically ill patients with AKI, to determine whether the accelerated initiation of RRT reduces mortality compared to a strategy of standard RRT initiation whereby RRT is initiated if urgent complications of AKI arise or based on clinician judgment.
Pragmatic allocation-concealed open-label randomized controlled trial.
Up to 170 centers in Australia, Austria, Belgium, Brazil, Canada, China, France, Germany, Ireland, Italy, Finland, New Zealand, Switzerland, the United Kingdom, and the United States.
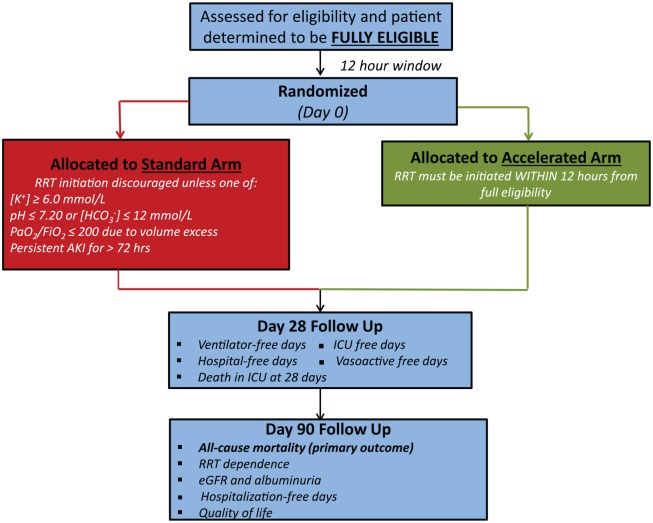
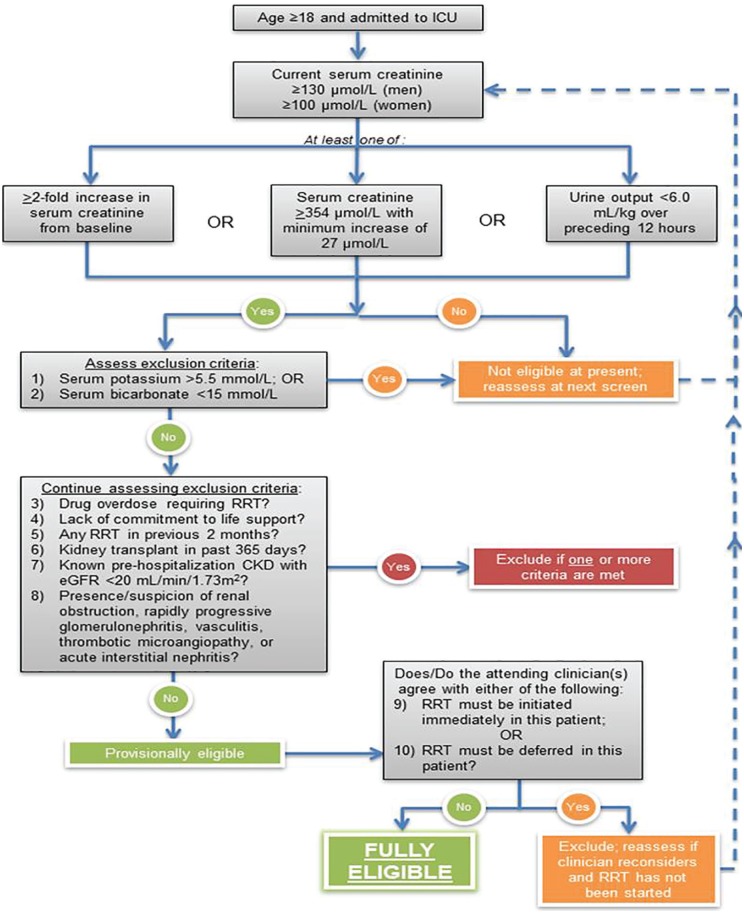
We will enroll at least 2,866 critically ill patients with AKI stages 2 or 3 (defined as doubling of serum creatinine from baseline or serum creatinine ≥354 µmol/L with increase of ≥27 µmol/L from baseline or urine output <6 mL/kg in preceding 12 hours). Patients will be excluded if 1 or more of the following is/are present: potassium >5.5 mmol/L; bicarbonate <15 mmol/L; concomitant intoxication necessitating RRT; philosophy of care precluding escalation to RRT; any RRT in preceding 2 months; kidney transplant within the past year; preexisting estimated glomerular filtration rate <20 mL/min/1.73 m; AKI etiology attributable to obstruction, glomerulonephritis, vasculitis, microangiopathy, or acute interstitial nephritis; clinician opinion that urgent RRT is mandated; or clinician opinion that RRT must be deferred.
Participants will be randomized to one of two strategies: accelerated RRT initiation, which entails the initiation of RRT within 12 hours of the patient fulfilling all eligibility criteria, or standard RRT initiation, whereby clinicians would be discouraged from initiating RRT unless a conventional trigger for RRT initiation arises or if AKI persists for ≥72 hours.
The primary outcome is all-cause mortality at 90 days following randomization. Key secondary outcomes include RRT dependence, residual kidney function, health services use, and health-related quality of life, all assessed at 90 days after randomization. In jurisdictions where it is feasible, participants will be followed through day 365 using linked administrative data.
Through March 18, 2019, we have recruited 2623 (92% of target) participants.
Reliance on physician declaration of equipoise may create heterogeneity across the trial population; open-label design may introduce bias and uneven postrandomization cointerventions; variations in practice (eg, choice of RRT modality and RRT prescription) likely exist across sites.
Once complete, the STARRT-AKI trial will provide the most robust evidence to date to guide clinical practice on the optimal timing of RRT initiation among critically ill patients with AKI.
Clinicaltrials.gov NCT02568722.
急性肾损伤(AKI)危重症患者开始肾脏替代治疗(RRT)的最佳时机仍存在争议。
在AKI危重症患者中,确定与标准RRT启动策略相比,加速启动RRT是否能降低死亡率。标准RRT启动策略是在出现AKI紧急并发症时或根据临床医生判断启动RRT。
实用的分配隐藏开放标签随机对照试验。
澳大利亚、奥地利、比利时、巴西、加拿大、中国、法国、德国、爱尔兰、意大利、芬兰、新西兰、瑞士、英国和美国的多达170个中心。
我们将招募至少2866例AKI 2期或3期危重症患者(定义为血清肌酐较基线水平翻倍或血清肌酐≥354 µmol/L且较基线水平升高≥27 µmol/L或前12小时尿量<6 mL/kg)。如果存在以下1项或多项情况,则排除患者:血钾>5.5 mmol/L;碳酸氢盐<15 mmol/L;需要RRT的合并中毒;护理理念不允许升级至RRT;前2个月内进行过任何RRT;过去一年内进行过肾移植;既往估计肾小球滤过率<20 mL/min/1.73 m²;AKI病因归因于梗阻、肾小球肾炎、血管炎、微血管病或急性间质性肾炎;临床医生认为必须紧急进行RRT;或临床医生认为必须推迟RRT。
参与者将被随机分配到两种策略之一:加速RRT启动,即在患者符合所有入选标准后12小时内启动RRT;或标准RRT启动,即除非出现RRT启动的传统触发因素或AKI持续≥72小时,否则不鼓励临床医生启动RRT。
主要结局是随机分组后90天的全因死亡率。关键次要结局包括RRT依赖、残余肾功能、卫生服务利用和健康相关生活质量,均在随机分组后90天进行评估。在可行的司法管辖区,将使用关联的行政数据对参与者进行随访至365天。
截至2019年3月18日,我们已招募了2623名(占目标的92%)参与者。
依赖医生对 equipoise 的声明可能会在试验人群中产生异质性;开放标签设计可能会引入偏差和随机分组后不均衡的联合干预;各研究地点可能存在实践差异(例如,RRT模式和RRT处方的选择)。
一旦完成,STARRT-AKI试验将提供迄今为止最有力的证据,以指导AKI危重症患者RRT启动最佳时机的临床实践。
Clinicaltrials.gov NCT02568722。