Törnblom Sanna, Nisula Sara, Petäjä Liisa, Vaara Suvi T, Haapio Mikko, Pesonen Eero, Pettilä Ville
Division of Intensive Care Medicine, Department of Anaesthesiology, Intensive Care and Pain Medicine, University of Helsinki and Helsinki University Hospital, PO Box 340, 00029 HUS, Helsinki, Finland.
Division of Anaesthesiology, Department of Anaesthesiology, Intensive Care and Pain Medicine, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
Ann Intensive Care. 2020 Apr 28;10(1):51. doi: 10.1186/s13613-020-00667-7.
Neutrophil gelatinase-associated lipocalin (NGAL) is released from kidney tubular cells under stress as well as from neutrophils during inflammation. It has been suggested as a biomarker for acute kidney injury (AKI) in critically ill patients with sepsis. To evaluate clinical usefulness of urine NGAL (uNGAL), we post-hoc applied recently introduced statistical methods to a sub-cohort of septic patients from the prospective observational Finnish Acute Kidney Injury (FINNAKI) study. Accordingly, in 484 adult intensive care unit patients with sepsis by Sepsis-3 criteria, we calculated areas under the receiver operating characteristic curves (AUCs) for the first available uNGAL to assess discrimination for four outcomes: AKI defined by Kidney Disease: Improving Global Outcomes (KDIGO) criteria, severe (KDIGO 2-3) AKI, and renal replacement therapy (RRT) during the first 3 days of intensive care, and mortality at day 90. We constructed clinical prediction models for the outcomes and used risk assessment plots and decision curve analysis with predefined threshold probabilities to test whether adding uNGAL to the models improved reclassification or decision making in clinical practice.
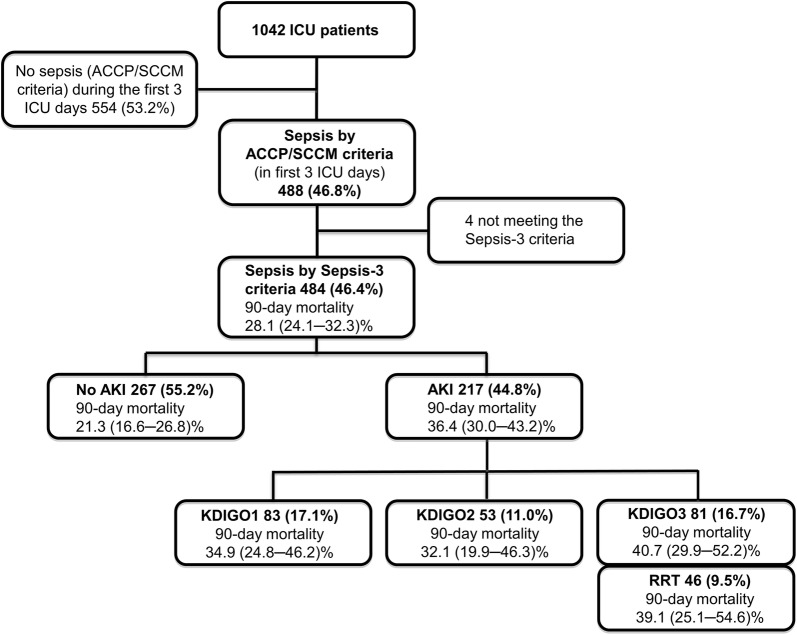
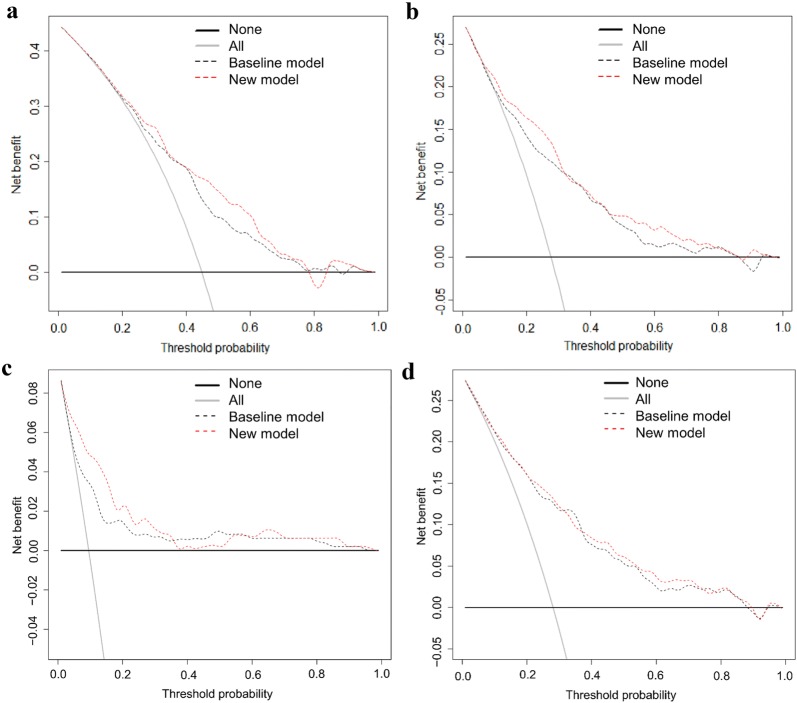
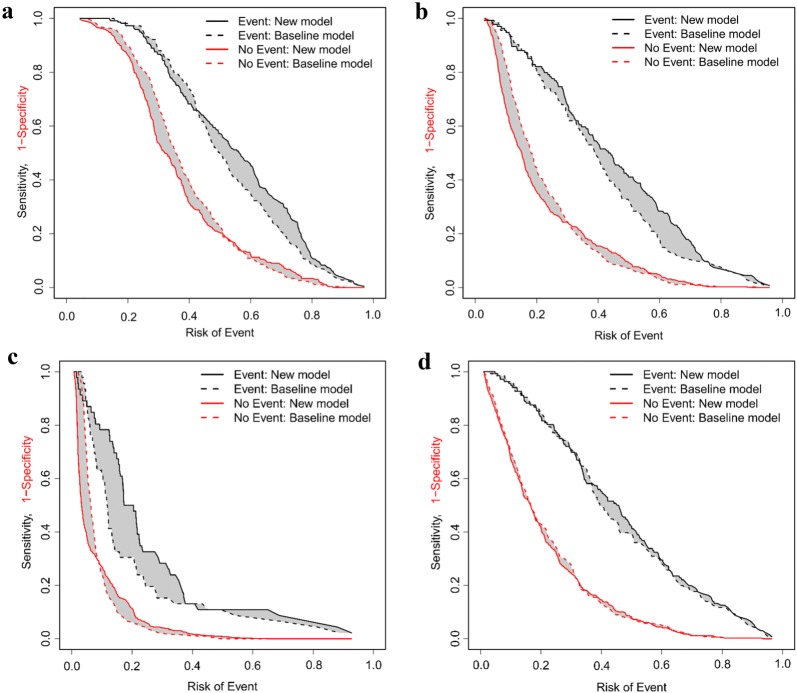
Incidences of AKI, severe AKI, RRT, and mortality were 44.8% (217/484), 27.7% (134/484), 9.5% (46/484), and 28.1% (136/484). Corresponding AUCs for uNGAL were 0.690, 0.728, 0.769, and 0.600. Adding uNGAL to the clinical prediction models improved discrimination of AKI, severe AKI, and RRT. However, the net benefits for the new models were only 1.4% (severe AKI and RRT) to 2.5% (AKI), and the number of patients needed to be tested per one extra true-positive varied from 40 (AKI) to 74 (RRT) at the predefined threshold probabilities.
The results of the recommended new statistical methods do not support the use of uNGAL in critically ill septic patients to predict AKI or clinical outcomes.
中性粒细胞明胶酶相关脂质运载蛋白(NGAL)在应激状态下可从肾小管细胞释放,在炎症过程中也可从中性粒细胞释放。它被认为是脓毒症重症患者急性肾损伤(AKI)的生物标志物。为评估尿NGAL(uNGAL)的临床实用性,我们对前瞻性观察性芬兰急性肾损伤(FINNAKI)研究中的一部分脓毒症患者进行事后分析,应用了最近引入的统计方法。因此,在484例符合脓毒症-3标准的成人重症监护病房患者中,我们计算了首次可获得的uNGAL的受试者工作特征曲线下面积(AUC),以评估其对以下四种结局的判别能力:根据改善全球肾脏病预后(KDIGO)标准定义的AKI、重度(KDIGO 2-至3期)AKI、重症监护前3天内的肾脏替代治疗(RRT)以及90天时的死亡率。我们构建了这些结局的临床预测模型,并使用风险评估图和决策曲线分析以及预定义的阈值概率来测试将uNGAL添加到模型中是否能改善临床实践中的重新分类或决策制定。
AKI、重度AKI、RRT和死亡率的发生率分别为44.8%(217/484)、27.7%(134/484)、9.5%(46/484)和28.1%(136/484)。uNGAL对应的AUC分别为0.690、0.728、0.769和0.600。将uNGAL添加到临床预测模型中可改善对AKI、重度AKI和RRT的判别能力。然而,新模型的净效益仅为1.4%(重度AKI和RRT)至2.5%(AKI),在预定义的阈值概率下,每多一个真阳性所需检测的患者数量从40例(AKI)到74例(RRT)不等。
推荐的新统计方法的结果不支持在脓毒症重症患者中使用uNGAL来预测AKI或临床结局。