Université Laval Cancer Research Center 11, Côte du Palais, Quebec City, QC, Canada.
Research Center of the CHU de Québec-Université Laval (Oncology division), Côte du palais, Quebec City, QC, Canada.
PLoS One. 2019 Jun 20;14(6):e0218621. doi: 10.1371/journal.pone.0218621. eCollection 2019.
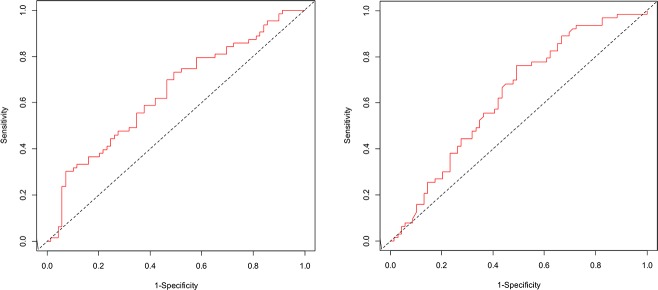
Clinical utility of new biomarkers often requires the identification of their optimal threshold. This external validation study was conducted to assess the performance of the preoperative plasma tumor markers HE4 and CA125 optimal cut-offs to predict cancer mortality in women with epithelial ovarian cancer (EOC). Participating women had upfront debulking surgery in the University Hospital of Quebec City (Canada) between 1998 and 2013. A total of 136 women participated in the training cohort (cohort 1) and 177 in the validation cohort (cohort 2). Preoperative plasma HE4 and CA125 levels were measured by Elecsys. Optimal thresholds were identified in the cohort 1 using time-dependent receiver operating characteristic (ROC) curves. Multivariate Cox models were used to validate the biomarkers using their optimal cut-offs in the cohort 2. The likelihood ratio (LR) test was done to test whether the biomarkers added prognostic information beyond that provided by standard prognostic factors. The Areas Under the Curves (AUC) for HE4 and CA125 were respectively 64.2 (95% CI: 54.7-73.6) and 63.1 (95%CI: 53.6-72.6). The optimal thresholds were 277 pmol/L for HE4 and 282 U/ml for CA125. Preoperative plasma HE4 (≥277 pmol/L) was significantly associated with EOC mortality (adjusted hazard ratio (aHR): 1.90; 95% CI:1.09-3.29). The prognostic effect of HE4 was strongest in the subgroup of women with serous ovarian cancer (aHR: 2.42; 95% CI: 1.25-4.68). Using a multivariate model including all standard prognostic factors, this association was maintained (aHR: 2.21; 95% CI: 1.15-4.23). In addition, preoperative plasma HE4 added prediction for death over the standard prognostic markers in women with serous tumors (p-value for LR-test: 0.01). Preoperative CA125 was not associated with cancer mortality, both in women with EOC and in those with serous tumors. Preoperative HE4 is a promising prognostic biomarker in EOC, especially in serous tumor.
新生物标志物的临床实用性通常需要确定其最佳阈值。本外部验证研究旨在评估术前血浆肿瘤标志物 HE4 和 CA125 最佳截断值预测上皮性卵巢癌(EOC)女性癌症死亡率的性能。参与研究的女性于 1998 年至 2013 年在魁北克城大学医院(加拿大)进行了初次减瘤手术。共有 136 名女性参加了训练队列(队列 1),177 名女性参加了验证队列(队列 2)。术前血浆 HE4 和 CA125 水平通过 Elecsys 进行测量。使用时间依赖性接受者操作特征(ROC)曲线在队列 1 中确定最佳截断值。使用队列 2 中的最佳截断值,使用多变量 Cox 模型验证生物标志物。似然比(LR)检验用于测试生物标志物是否提供了标准预后因素之外的预后信息。HE4 和 CA125 的曲线下面积(AUC)分别为 64.2(95%CI:54.7-73.6)和 63.1(95%CI:53.6-72.6)。最佳截断值分别为 277 pmol/L 用于 HE4 和 282 U/ml 用于 CA125。术前血浆 HE4(≥277 pmol/L)与 EOC 死亡率显著相关(调整后的危险比(aHR):1.90;95%CI:1.09-3.29)。HE4 的预后作用在浆液性卵巢癌女性亚组中最强(aHR:2.42;95%CI:1.25-4.68)。使用包含所有标准预后因素的多变量模型,这种关联仍然存在(aHR:2.21;95%CI:1.15-4.23)。此外,在浆液性肿瘤女性中,术前血浆 HE4 增加了对标准预后标志物的死亡预测(LR 检验的 p 值:0.01)。术前 CA125 与 EOC 女性和浆液性肿瘤女性的癌症死亡率均无关。术前 HE4 是 EOC 中一种很有前途的预后生物标志物,特别是在浆液性肿瘤中。