School of Social Sciences, Bangor University, Room 107, Neuaddc Ogwen, Bangor, Wales, UK, LL57 2DG.
Major Health Conditions Policy Team, Directorate of Health Policy, Health and Social Services Group, Welsh Government, Cardiff, Wales, UK, CF10 3NQ.
BMC Health Serv Res. 2019 Jun 24;19(1):414. doi: 10.1186/s12913-019-4266-z.
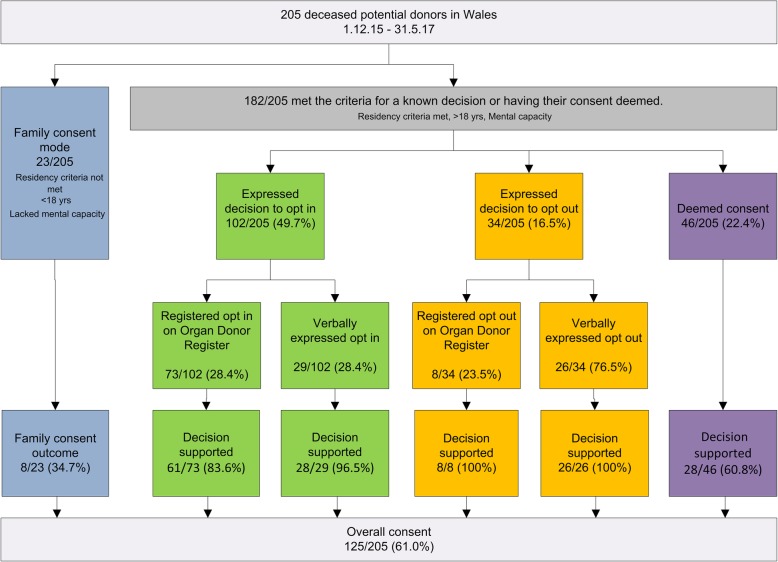
Wales introduced a soft opt-out organ donation system on 1st December 2015 with the aim of improving consent rates. In the first 18 months consent rates improved but the difference could not solely be attributed to the soft opt-out system when compared with similar improvements in consent rates in other UK nations.
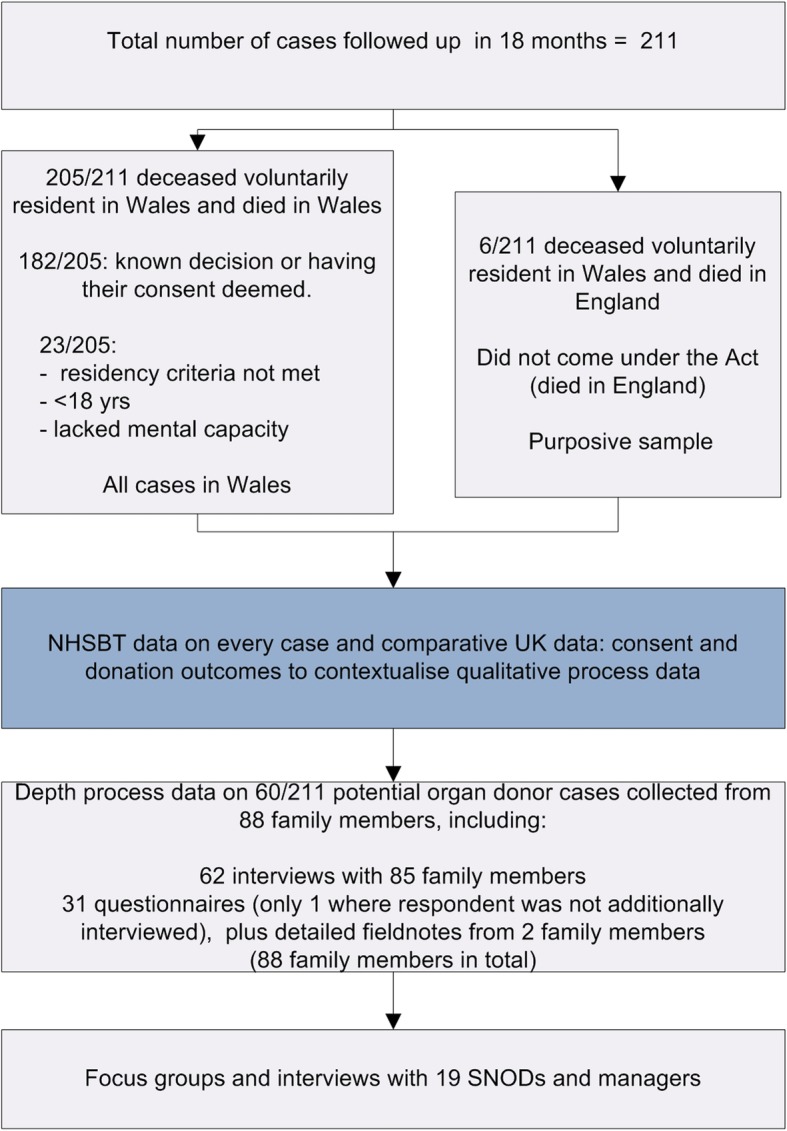
We conducted an 18 month post-intervention qualitative process evaluation involving 88 family members of 60/211 potential organ donor cases, and 19 professionals. Views and experiences of Specialist Nurses in Organ Donation who implemented the new system and family members who were involved in decision making were collected to see how their respective behaviours impacted on implementation. Data collection included interviews, focus groups and qualitative questionnaire data.
Implementation was considered a success by Specialist Nurses in Organ Donation. The bespoke retraining programme and responsive approach to addressing initial implementation issues were identified as examples of best practice. Specialist Nurses in Organ Donation were valued by family members. Six implementation issues had an impact on consent rates - the media campaign had gaps, the system was more complex, challenges in changing professional behaviours, inability to obtain the required standard of evidence from family members to overturn a donation decision, increased complexity of consent processes, and additional health systems issues.
This is the first comprehensive process evaluation of implementing a soft opt-out system of organ donation. Specific elements of good implementation practice (such as investment in the retraining programme and the responsiveness of Specialist Nurses in Organ Donation and managers to feedback) were identified. The key message is that despite retraining, nursing practice did not radically change overnight to accommodate the new soft opt-out system. Policy makers and health service managers should not assume that nurses simply need more time to implement the soft-out as intended. Additional responsive modification of processes, ongoing training and support is required to help with implementation as originally intended. Scotland, England and the Netherlands are introducing soft opt-out systems. There is an opportunity to learn from initial implementation in Wales, by acknowledging gaps, good practice and opportunities to further improve processes and nursing practices.
威尔士于 2015 年 12 月 1 日引入了软性默认器官捐献系统,旨在提高同意率。在前 18 个月中,同意率有所提高,但与其他英国国家同意率的类似提高相比,这一差异不能完全归因于软性默认系统。
我们进行了一项为期 18 个月的干预后定性过程评估,涉及 60/211 名潜在器官捐献者案例的 88 名家属和 19 名专业人员。收集了实施新系统的器官捐献专家护士以及参与决策的家属的意见和经验,以了解他们各自的行为如何影响实施。数据收集包括访谈、焦点小组和定性问卷数据。
器官捐献专家护士认为实施取得了成功。专门的再培训计划和解决初始实施问题的响应方法被确定为最佳实践的例子。器官捐献专家护士受到家属的重视。有六个实施问题对同意率产生了影响——媒体宣传存在漏洞,系统更加复杂,改变专业行为的挑战,无法从家属那里获得推翻捐赠决定所需的证据标准,同意程序的复杂性增加,以及额外的卫生系统问题。
这是首次对实施软性默认器官捐献系统进行全面的过程评估。确定了一些良好实施实践的具体要素(例如对再培训计划的投资以及器官捐献专家护士和管理人员对反馈的响应能力)。关键信息是,尽管进行了再培训,护理实践并没有在一夜之间彻底改变以适应新的软性默认系统。政策制定者和卫生服务管理者不应假设护士只需要更多的时间来按照软性默认系统的预期实施。需要进行额外的响应式流程修改、持续培训和支持,以帮助按照最初的意图进行实施。苏格兰、英格兰和荷兰正在引入软性默认系统。有机会通过承认差距、良好实践和进一步改进流程和护理实践的机会,从威尔士的初步实施中吸取经验。