Tonelli Marcello, Wiebe Natasha, Richard Jean-Francois, Klarenbach Scott W, Hemmelgarn Brenda R
Department of Medicine, University of Calgary, Calgary, AB, Canada.
Department of Medicine, University of Alberta, Edmonton, AB, Canada.
Can J Kidney Health Dis. 2019 Jun 13;6:2054358119854113. doi: 10.1177/2054358119854113. eCollection 2019.
Type 2 diabetes mellitus (T2DM) is associated with an excess risk of cardiovascular disease (CVD) and chronic kidney disease (CKD). Although CVD, CKD, and use of antihyperglycemic treatments are all key drivers of the costs and consequences experienced by people with diabetes, no recent Canadian data describe these characteristics among adults with diabetes.
To describe prevalence of CVD, CKD, and use of antihyperglycemic treatments among adults with diabetes.
Retrospective population-based, cross-sectional study.
Alberta, Canada.
All adults with T2DM as of March 31, 2017.
We described the demographic and clinical characteristics by CKD stage and CVD status and type. CKD stage was categorized according to international guidelines and based on estimated glomerular filtration rate (eGFR) and severity of albuminuria.
Clinical and demographic characteristics were defined using provincial administrative data; medication use was based on data from the provincial drug plan. Additional analyses examined subgroups based on demographic characteristics, clinical characteristics, and medication use.
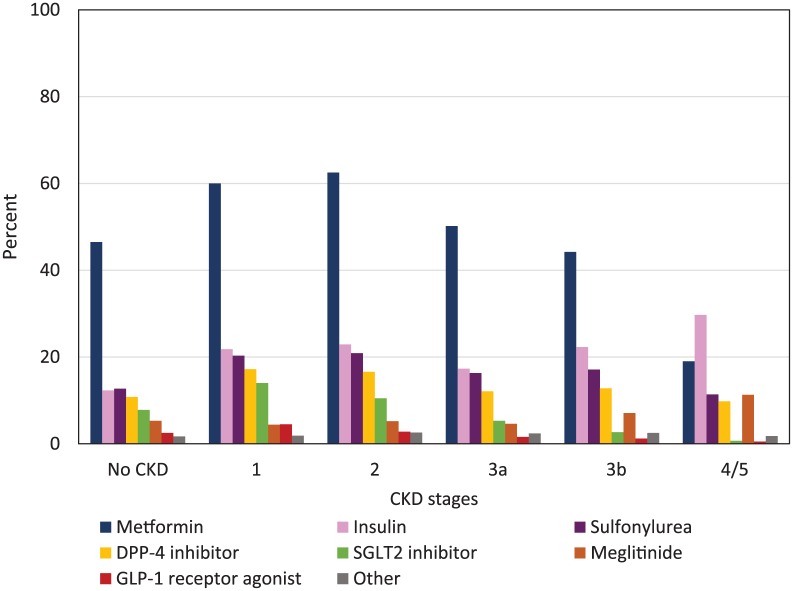
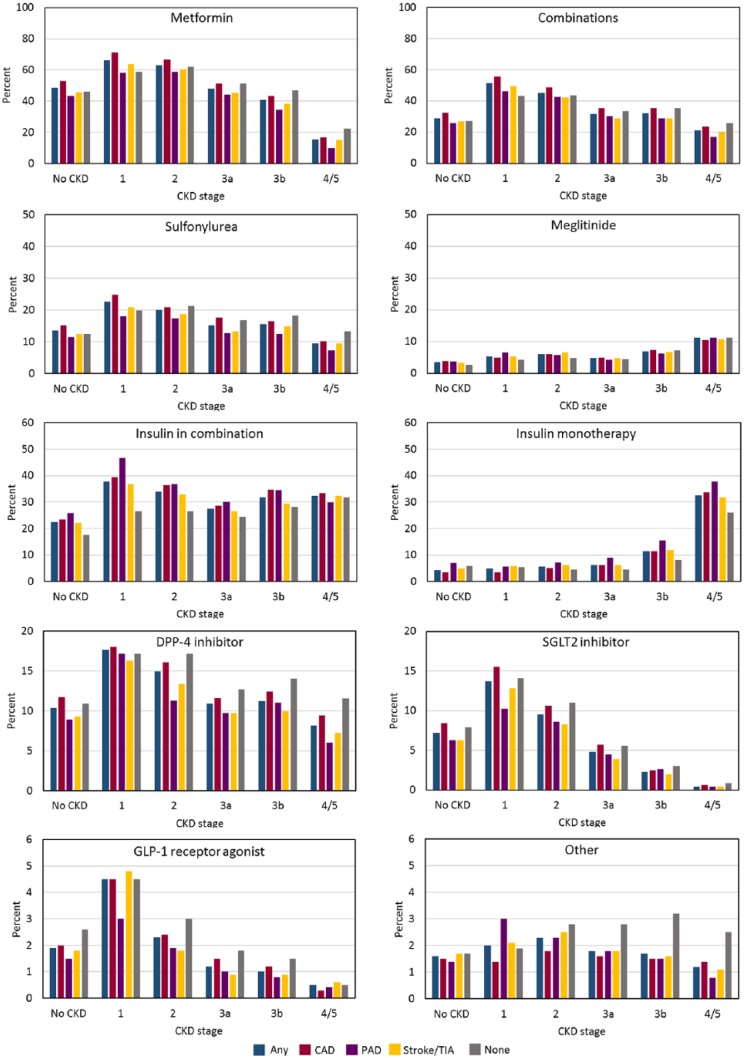
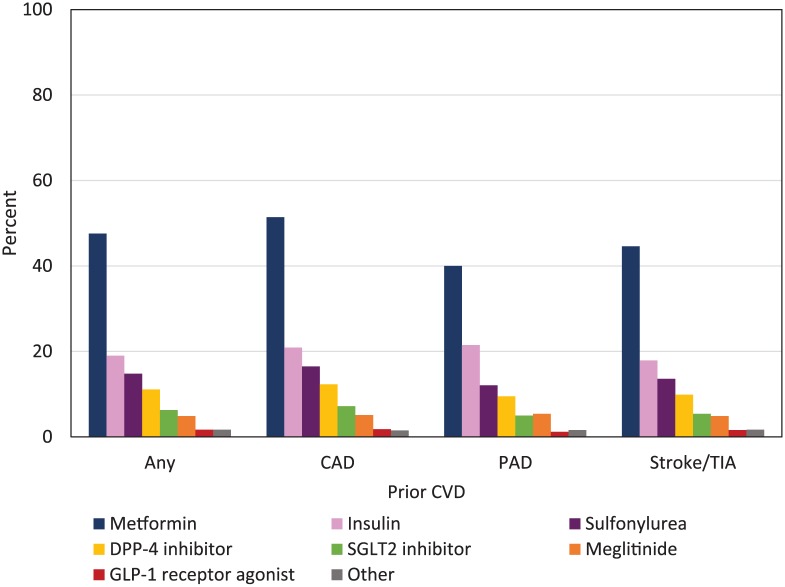
There were 260 903 participants, all of whom had T2DM. Median age was 64 years; 53.6% were male; and 10.9% lived in rural communities. Median duration of diabetes was 7.7 years. Half of the participants had A1C <7%. Overall, 33.0% had CKD; among these most had eGFR <60 mL/min/1.73 m; 11.1%, 5.6%, and 2.9% had CKD stages 3a, 3b, and 4/5, respectively. The overall prevalence of CVD (prior myocardial infarction, stroke/transient ischemic attack, or peripheral artery disease) was 22.5%; prevalence increased in parallel with the presence of CKD: 14.4%, 28.8%, 35.7%, 44.3%, and 50.9% for stages 1, 2, 3a, 3b, and 4/5, respectively. Prescriptions for antihyperglycemic medications were more common in people with CKD as compared with those without. However, the use of all antihyperglycemic medications except insulin and meglitinide was progressively lower in the presence of more severe CKD.
The study is based on administrative data; therefore, the findings could be influenced by measurement error (eg, accuracy of diagnostic and procedural codes and prescription drug codes used).
These findings will be useful to policy makers seeking to understand the burden of diabetes-related kidney disease as well as the potential budget implications and potential clinical benefits of expanded use of antihyperglycemic use in this population.
2型糖尿病(T2DM)与心血管疾病(CVD)和慢性肾脏病(CKD)风险增加相关。尽管CVD、CKD以及降糖治疗的使用都是糖尿病患者所经历的成本和后果的关键驱动因素,但最近没有加拿大的数据描述糖尿病成年人的这些特征。
描述糖尿病成年人中CVD、CKD的患病率以及降糖治疗的使用情况。
基于人群的回顾性横断面研究。
加拿大艾伯塔省。
截至2017年3月31日的所有成年T2DM患者。
我们按CKD分期、CVD状态和类型描述了人口统计学和临床特征。CKD分期根据国际指南,基于估计肾小球滤过率(eGFR)和蛋白尿严重程度进行分类。
使用省级行政数据定义临床和人口统计学特征;药物使用基于省级药物计划的数据。进一步分析根据人口统计学特征、临床特征和药物使用情况检查亚组。
共有260903名参与者,均患有T2DM。中位年龄为64岁;53.6%为男性;10.9%生活在农村社区。糖尿病中位病程为7.7年。一半的参与者糖化血红蛋白(A1C)<7%。总体而言,33.0%的人患有CKD;其中大多数人的eGFR<60 mL/min/1.73 m²;CKD 3a期、3b期和4/5期的患者分别占11.1%、5.6%和2.9%。CVD(既往心肌梗死、中风/短暂性脑缺血发作或外周动脉疾病)的总体患病率为22.5%;患病率随CKD的存在而平行增加:1期、2期、3a期、3b期和4/5期的患病率分别为14.4%、28.8%、35.7%、44.3%和50.9%。与未患CKD的人相比,CKD患者中降糖药物处方更常见。然而,在更严重的CKD患者中,除胰岛素和格列奈类药物外,所有降糖药物的使用都逐渐减少。
本研究基于行政数据;因此,研究结果可能受到测量误差(如所用诊断和程序代码以及处方药代码的准确性)的影响。
这些发现将有助于政策制定者了解糖尿病相关肾脏疾病的负担,以及在该人群中扩大使用降糖药物的潜在预算影响和潜在临床益处。