Department of Medicine, University of Alberta, 13-103 Clinical Sciences Building, 11350-83 Avenue, Edmonton, Alberta, T6G 2G3, Canada.
Department of Public Health, University of Missouri, 510 Lewis Hall, Columbia, MO, 65211, USA.
BMC Prim Care. 2022 May 24;23(1):124. doi: 10.1186/s12875-022-01731-w.
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1RA) have shown benefits in patients with diabetes and cardiovascular disease (CVD), heart failure (HF), and chronic kidney disease (CKD).
We assessed benchmark outcomes (Hemoglobin A1c, LDL-C, and blood pressure), identified the prevalence of cardiorenal indications for SGLT2i and GLP-1RA, and compared prescribing rates of GLP1-RA and SGLT2i in those with and without cardiorenal indications.
We analyzed data from January 2018-June 2019 for 7168 patients with diabetes using electronic medical records from the Northern Alberta Primary Care Research Network, a regional network of the Canadian Primary Sentinel Surveillance Network (CPCSSN). Patients with and without cardiorenal comorbidities were compared using descriptive statistics and two proportion Z tests.
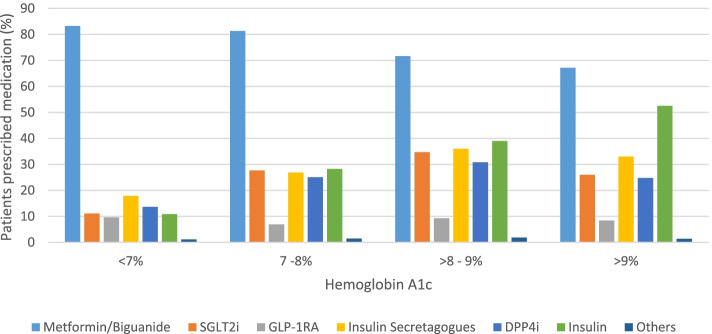
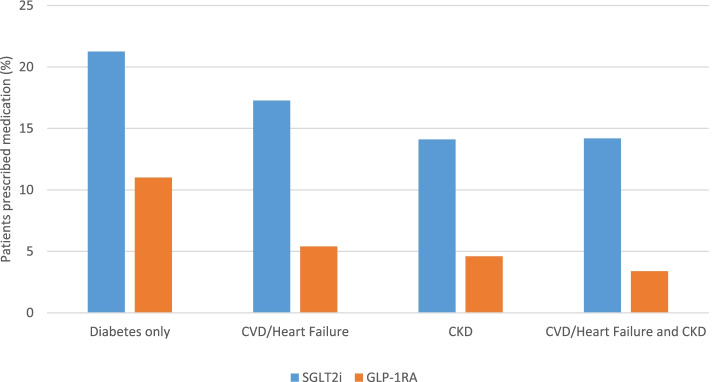
Hemoglobin A1c ≤ 7.0% was met by 56.8%, blood pressure < 130/80 mmHg by 62.1%, LDL-C ≤ 2.0 mmol/L by 45.3% of patients. There were 4377 patients on glucose lowering medications; metformin was most common (77.7%), followed by insulin (24.6%), insulin secretagogues (23.6%), SGLT2i (19.7%), dipeptidyl peptidase-4 inhibitor (19.3%), and GLP-1RA (9.4%). A quarter of patients had cardiorenal indications for SGLT2i or GLP-1RA. Use of SGLT2i in these patients was lower than in patients without cardiorenal comorbidities (14.9% vs 21.2%, p < 0.05). GLP-1RA use in these patients was 4.6% compared with 11% in those without cardiorenal comorbidities (p < 0.05).
Contrary to current evidence and recommendations, SGLT2i and GLP1-RA were less likely to be prescribed to patients with pre-existing CVD, HF, and/or CKD, revealing opportunities to improve prescribing for patients with diabetes at high-risk for worsening cardiorenal complications.
钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)和胰高血糖素样肽-1 受体激动剂(GLP-1RA)已显示出对糖尿病和心血管疾病(CVD)、心力衰竭(HF)和慢性肾脏病(CKD)患者的益处。
我们评估了基准结局(糖化血红蛋白、LDL-C 和血压),确定了 SGLT2i 和 GLP-1RA 的心脏肾脏适应证的患病率,并比较了有和没有心脏肾脏适应证的患者中 GLP1-RA 和 SGLT2i 的处方率。
我们使用加拿大初级监测网络(CPCSSN)的区域网络——加拿大北阿尔伯塔初级保健研究网络的电子病历,分析了 2018 年 1 月至 2019 年 6 月期间 7168 名糖尿病患者的数据。使用描述性统计和两比例 Z 检验比较了有和无心脏肾脏合并症的患者。
56.8%的患者糖化血红蛋白≤7.0%,62.1%的患者血压<130/80mmHg,45.3%的患者 LDL-C≤2.0mmol/L。有 4377 名患者使用降血糖药物;最常见的是二甲双胍(77.7%),其次是胰岛素(24.6%)、胰岛素促分泌剂(23.6%)、SGLT2i(19.7%)、二肽基肽酶-4 抑制剂(19.3%)和 GLP-1RA(9.4%)。四分之一的患者有 SGLT2i 或 GLP-1RA 的心脏肾脏适应证。在这些患者中,SGLT2i 的使用低于无心脏肾脏合并症的患者(14.9%比 21.2%,p<0.05)。在这些患者中,GLP-1RA 的使用为 4.6%,而无心脏肾脏合并症的患者为 11%(p<0.05)。
与当前的证据和建议相反,SGLT2i 和 GLP1-RA 不太可能被开给患有预先存在的 CVD、HF 和/或 CKD 的患者,这表明有机会改善高危发生心脏肾脏并发症的糖尿病患者的处方。