Hernández-Madrid Antonio, Lu Xiaoxiao, Tsintzos Stelios I, Fagan Dedra H, Klepfer Ruth Nicholson, Matía Roberto, Chung Eugene S
Arrhythmia Unit, Cardiology Department, Ramón y Cajal Hospital, Alcalá University, Madrid, Spain.
Medtronic, plc, Mounds View, MN, USA.
Clinicoecon Outcomes Res. 2019 Jun 6;11:385-393. doi: 10.2147/CEOR.S205501. eCollection 2019.
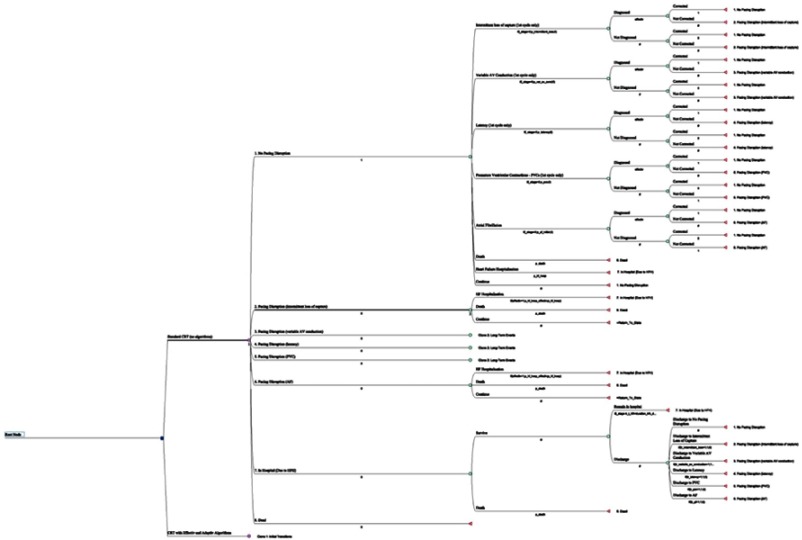
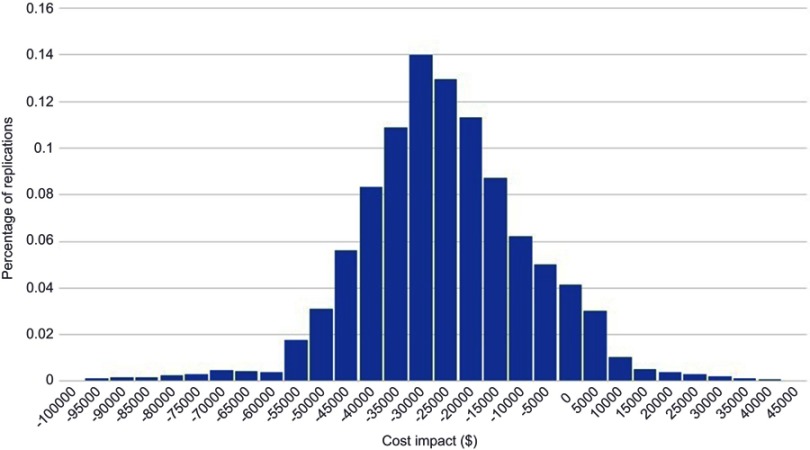
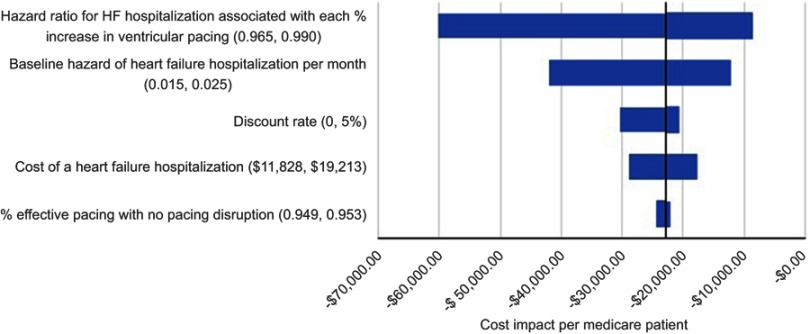
The hOLter for Efficacy analysis (OLE) study demonstrated that current device pacing diagnostics overestimate the amount of cardiac resynchronization therapy (CRT) pacing that effectively stimulates the cardiac tissue. Sub-optimal pacing increases mortality, hospitalizations, and associated health-care costs. We sought to estimate the expected number of hospital admissions due to heart failure (HF) and its respective financial impact in patients with maximized effective pacing versus conventional pacing. A Markov model was developed to project HF hospitalizations and quantify the costs that could be avoided if pacing was maximally effective. OLE data were used to inform the prevalence of ineffective pacing among CRT patients and and average loss of pacing by causes. Adaptive CRT trial data quantified the reduction in underlying hospitalization risk by increasing effective pacing delivered. Survival was informed by a meta-analysis of 5 randomized clinical trials. Costs were analyzed from a US payer perspective. Projected average hospitalizations totaled 4.58 over a lifetime horizon for CRT patients with conventional pacing. Maximizing effective pacing delivery was projected to avoid 1.83 HF admissions/patient over the lifetime. This equates to a savings of 40% (US$22,802) compared with conventional pacing from the Medicare perspective. In a sensitivity analysis, CRT with effective pacing was projected to provide cost savings in all scenarios. Maximized effective pacing leads to a lower number of HF hospitalizations, thus allowing significant cost offsets in the US setting.
用于疗效分析的动态心电图监测(OLE)研究表明,当前设备的起搏诊断高估了能有效刺激心脏组织的心脏再同步治疗(CRT)起搏量。起搏效果欠佳会增加死亡率、住院率以及相关医疗保健成本。我们试图估算在有效起搏最大化的患者与传统起搏患者中,因心力衰竭(HF)导致的预期住院次数及其各自的财务影响。构建了一个马尔可夫模型来预测HF住院情况,并量化如果起搏达到最大有效性时可避免的成本。OLE数据用于了解CRT患者中无效起搏的患病率以及按病因划分的平均起搏损失。适应性CRT试验数据量化了通过增加有效起搏可降低的潜在住院风险。通过对5项随机临床试验的荟萃分析得出生存率情况。从美国医保支付方的角度分析成本。对于接受传统起搏的CRT患者,预计其一生的平均住院次数总计为4.58次。预计将有效起搏输送最大化可使每位患者一生避免1.83次HF住院。从医疗保险的角度来看,这相当于与传统起搏相比节省了40%(22,802美元)。在敏感性分析中,预计在所有情况下有效起搏的CRT都能节省成本。有效起搏最大化可减少HF住院次数,从而在美国环境下实现显著的成本抵消。