Division of Gastroenterology, Department of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Center for Clinical Epidemiology and Biostatistics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Am J Transplant. 2019 Dec;19(12):3319-3327. doi: 10.1111/ajt.15513. Epub 2019 Jul 17.
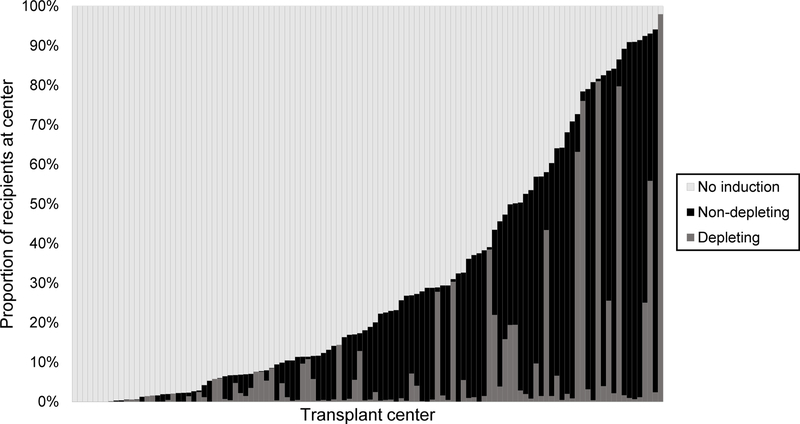
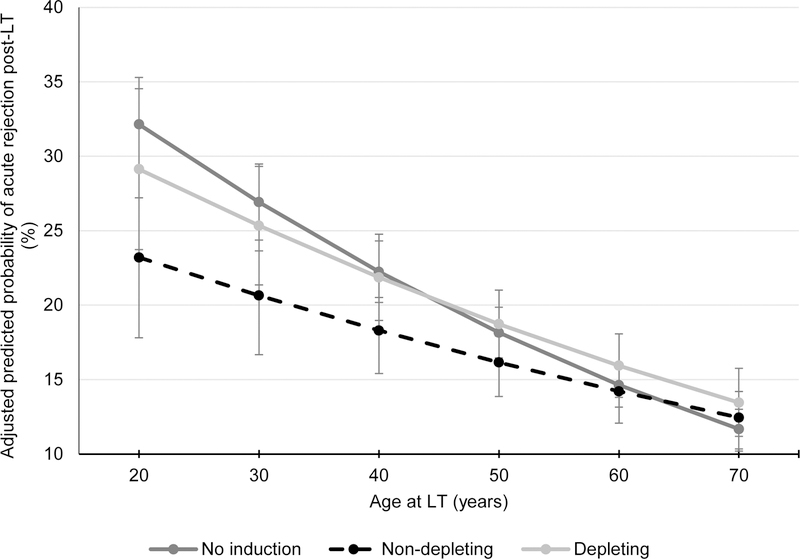
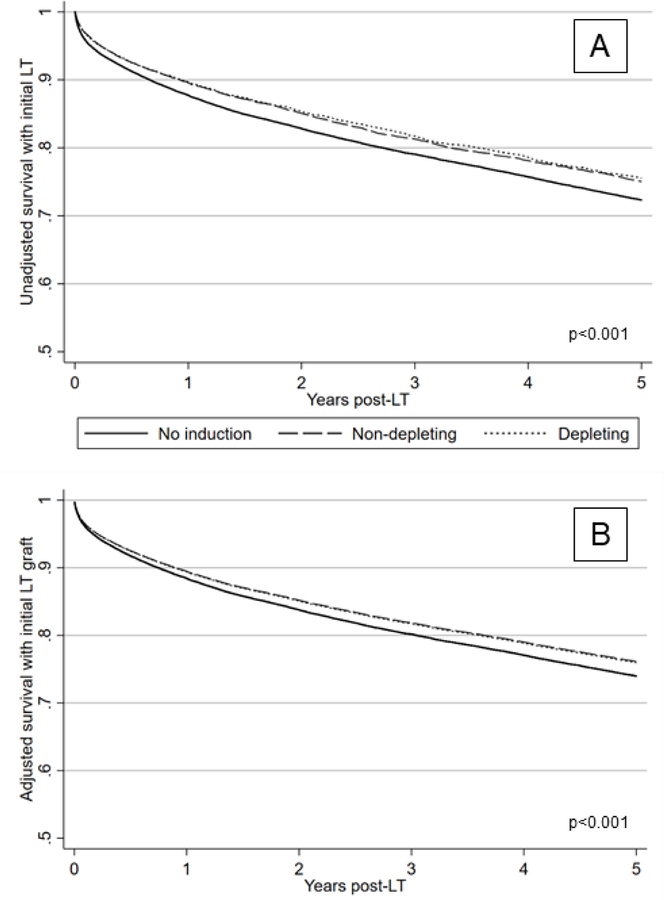
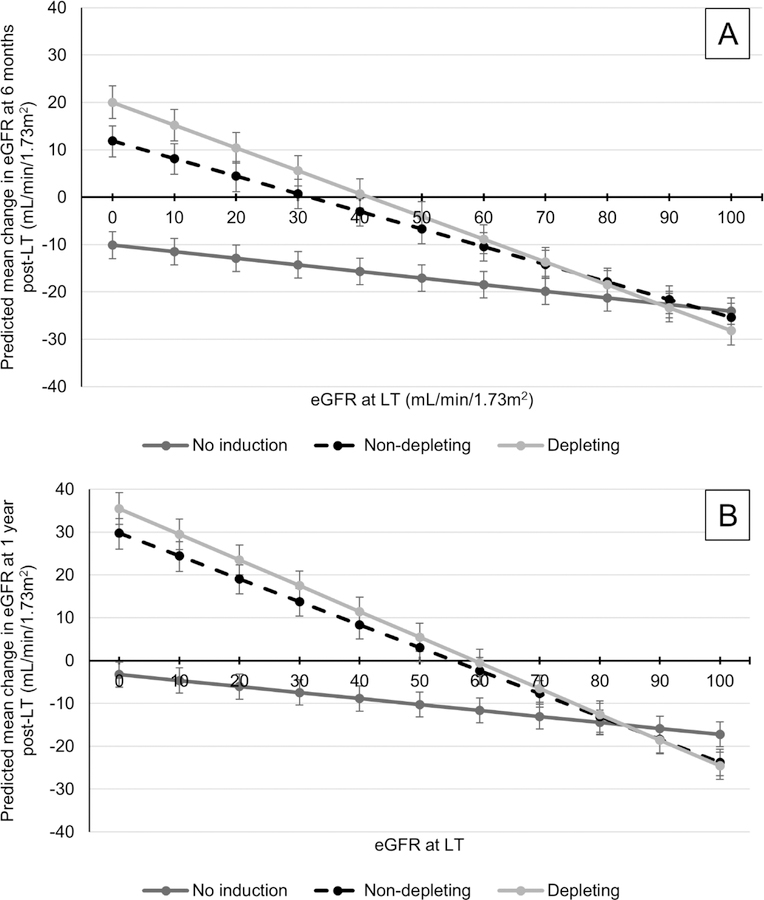
The use of induction immunosuppression in liver transplantation (LT) remains controversial. This was a retrospective cohort study of adult, first-time liver-alone recipients (N = 69 349) at 114 US centers between 2005 and 2018 using data from the United Network for Organ Sharing. The comparative effectiveness of nondepleting and depleting induction (NDI and DI) was assessed. Overall, 27% of recipients received induction with 65.7% of the variance in the receipt of induction being attributed to transplant center alone. NDI and DI were associated with a lower risk of death/graft failure compared to no induction (adjusted hazard ratio 0.90 [95% confidence interval (CI): 0.86-0.95] and 0.91 [95% CI: 0.85-0.97], respectively; P < .001). In nondialysis recipients at the mean transplant estimated glomerular filtration rate (eGFR), NDI was associated with an adjusted gain in eGFR by 6 months of +3.8 mL/min per 1.73 m and DI of +3.33 mL/min per 1.73 m compared to no induction (P < .001). Recipients with lower eGFR at LT had greater predicted improvement in eGFR (interaction P < .001). Only NDI was associated with a reduced risk of acute rejection in the first year post-LT (odds ratio 0.87, 95% CI: 0.8-0.94). Significant variability in induction practices exists, with center being a major determinant. The absolute incremental benefits of NDI and DI over no induction were small.
诱导免疫抑制在肝移植(LT)中的应用仍存在争议。这是一项回顾性队列研究,纳入了 2005 年至 2018 年间美国 114 个中心的 69349 例成人首次单独接受肝移植的患者,该研究使用了美国器官共享网络的数据。评估了非耗竭性和耗竭性诱导(NDI 和 DI)的比较效果。总体而言,27%的患者接受了诱导治疗,而诱导治疗的接受率的 65.7%归因于移植中心。与未接受诱导治疗相比,NDI 和 DI 与较低的死亡/移植物失败风险相关(校正后的危险比分别为 0.90[95%可信区间(CI):0.86-0.95]和 0.91[95%CI:0.85-0.97];P<.001)。在平均移植估计肾小球滤过率(eGFR)的非透析患者中,与未接受诱导治疗相比,NDI 可使 eGFR 在 6 个月时增加 3.8 mL/min/1.73 m,而 DI 可使 eGFR 增加 3.33 mL/min/1.73 m(P<.001)。LT 时 eGFR 较低的患者,eGFR 预测改善幅度更大(交互作用 P<.001)。只有 NDI 与 LT 后第一年急性排斥反应风险降低相关(比值比 0.87,95%CI:0.8-0.94)。诱导治疗实践存在显著差异,中心是主要决定因素。NDI 和 DI 与不诱导治疗相比,绝对增量获益较小。