Dieci Maria Vittoria, Tsvetkova Vassilena, Griguolo Gaia, Miglietta Federica, Mantiero Mara, Tasca Giulia, Cumerlato Enrico, Giorgi Carlo Alberto, Giarratano Tommaso, Faggioni Giovanni, Falci Cristina, Vernaci Grazia, Menichetti Alice, Mioranza Eleonora, Di Liso Elisabetta, Frezzini Simona, Saibene Tania, Orvieto Enrico, Guarneri Valentina
Department of Surgery, Oncology and Gastroenterology, University of Padova, Padova, Italy.
Medical Oncology 2, Istituto Oncologico Veneto IOV-IRCCS, Padova, Italy.
Front Oncol. 2019 Jun 6;9:452. doi: 10.3389/fonc.2019.00452. eCollection 2019.
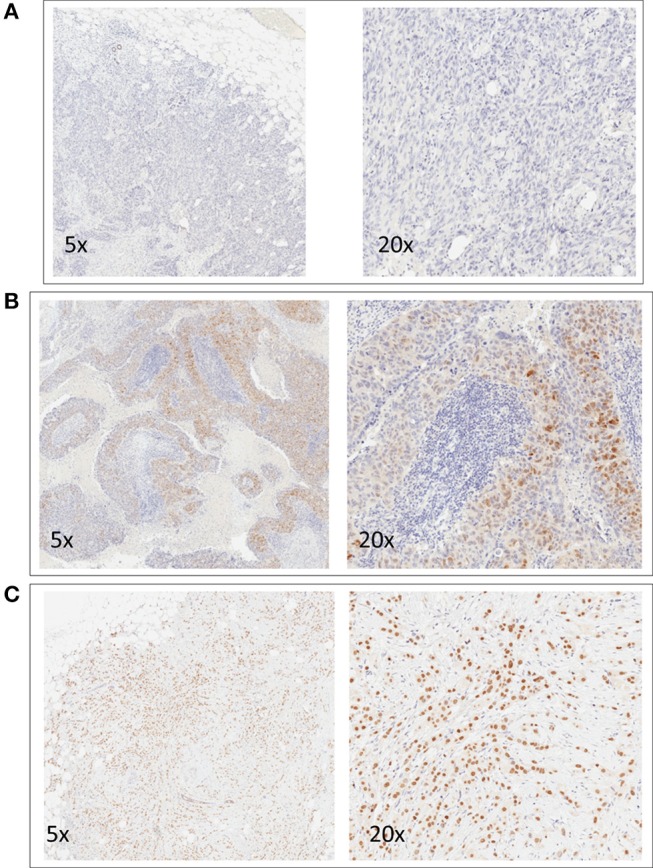
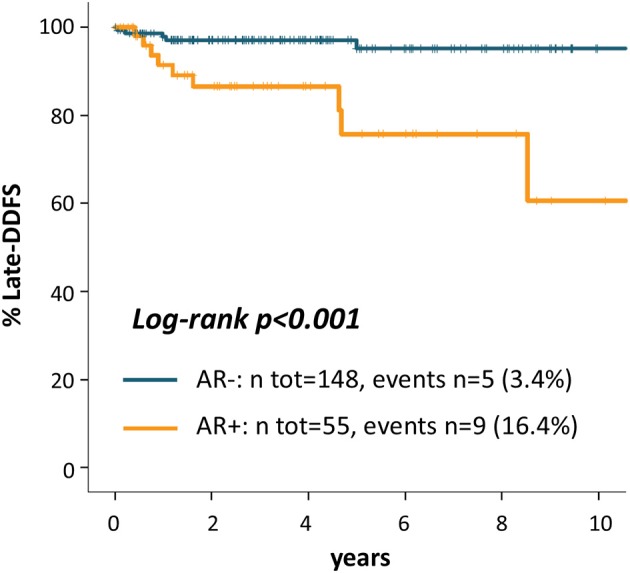
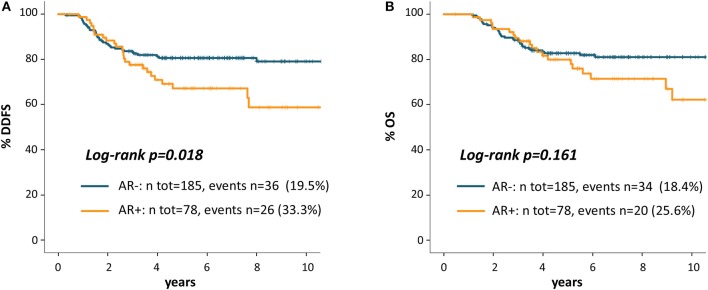
We evaluated immunohistochemical AR expression and correlation with prognosis in a large series of homogeneously treated patients with primary TNBC. Patients diagnosed with stage I-III TNBC between 2000 and 2015 at Istituto Oncologico Veneto who received treatment with surgery and neoadjuvant and/or adjuvant chemotherapy were included. Whole tissue slides were stained for AR. AR-positive expression was defined as >1% of positively stained tumor cells. Distant-disease-free survival (DDFS) was calculated from diagnosis to distant relapse or death. Late-DDFS was calculated from the landmark of 3 years after diagnosis until distant relapse or death. We included 263 primary TNBC patients. Mean AR expression was 14% (range 0-100%), and 29.7% ( = 78) of patients were AR+. AR+ vs. AR- cases presented more frequently older age ( < 0.001), non-ductal histology ( < 0.001), G1-G2 ( = 0.003), lower Ki67 ( < 0.001) and lower TILs ( = 0.008). At a median follow up of 81 months, 23.6% of patients experienced a DDFS event: 33.3% of AR+ and 19.5% of AR- patients ( = 0.015). 5 years DDFS rates were 67.2% and 80.6% for AR+ and AR- patients (HR = 1.82 95%CI 1.10-3.02, = 0.020). AR maintained an independent prognostic role beyond stage, but when TILs were added to the model only stage and TILs were independent prognostic factors. AR was the only factor significantly associated with late-DDFS: 16.4% of AR+ and 3.4% of AR- patients experienced a DDFS after the landmark of 3 years after diagnosis ( = 0.001). Late-DDFS rates at 5 years from the 3-year landmark were 75.8% for AR+ and 95.2% for AR- patients (log-rank < 0.001; HR = 5.67, 95%CI 1.90-16.94, = 0.002). AR expression is associated with worse outcome for patients with TNBC. In particular, AR+ TNBC patients are at increased risk of late DDFS events. These results reinforce the rationale of AR targeting in AR+ TNBC.
我们评估了大量接受同质化治疗的原发性三阴性乳腺癌(TNBC)患者的免疫组化雄激素受体(AR)表达及其与预后的相关性。纳入了2000年至2015年期间在威尼斯肿瘤研究所被诊断为I - III期TNBC且接受了手术及新辅助和/或辅助化疗的患者。对全组织切片进行AR染色。AR阳性表达定义为阳性染色肿瘤细胞>1%。远处无病生存期(DDFS)从诊断至远处复发或死亡进行计算。晚期DDFS从诊断后3年的时间节点开始计算直至远处复发或死亡。我们纳入了263例原发性TNBC患者。AR平均表达为14%(范围0 - 100%),29.7%(n = 78)的患者为AR阳性。AR阳性与AR阴性病例相比,更常出现年龄较大(P < 0.001)、非导管组织学类型(P < 0.001)、G1 - G2级(P = 0.003)、较低的Ki67(P < 0.001)和较低的肿瘤浸润淋巴细胞(TILs)(P = 0.008)。中位随访81个月时,23.6%的患者发生了DDFS事件:AR阳性患者为33.3%,AR阴性患者为19.5%(P = 0.015)。AR阳性和AR阴性患者的5年DDFS率分别为67.2%和80.6%(风险比[HR] = 1.82,95%置信区间[CI] 1.10 - 3.02,P = 0.020)。AR在分期之外仍具有独立的预后作用,但当将TILs纳入模型时,只有分期和TILs是独立的预后因素。AR是与晚期DDFS显著相关的唯一因素:16.4%的AR阳性和3.4%的AR阴性患者在诊断后3年的时间节点后发生了DDFS事件(P = 0.001)。从3年时间节点起5年的晚期DDFS率,AR阳性患者为75.8%,AR阴性患者为95.2%(对数秩检验P < 0.001;HR = 5.67,95%CI 1.90 - 16.94,P = 0.002)。AR表达与TNBC患者的较差预后相关。特别是,AR阳性的TNBC患者发生晚期DDFS事件的风险增加。这些结果强化了在AR阳性TNBC中靶向AR的理论依据。