Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, UK.
Indian J Med Res. 2019 Mar;149(3):369-375. doi: 10.4103/ijmr.IJMR_1419_18.
BACKGROUND & OBJECTIVE: Given that Ayushman Bharat Yojna was launched in 2018 in India, analysis of Rashtriya Swasthya Bima Yojna (RSBY) become relevant. The objective of this study was to examine the scheme design and the incentive structure under RSBY.
The study was conducted in the districts of Patiala and Yamunanagar in the States of Punjab and Haryana, respectively (2011-2013). The mixed method study involved review of key documents; 20 in-depth interviews of key stakeholders; 399 exit interviews of RSBY and non-RSBY beneficiaries in Patiala and 353 in Yamunanagar from 12 selected RSBY empanelled hospitals; and analysis of secondary databases from State nodal agencies and district medical officers.
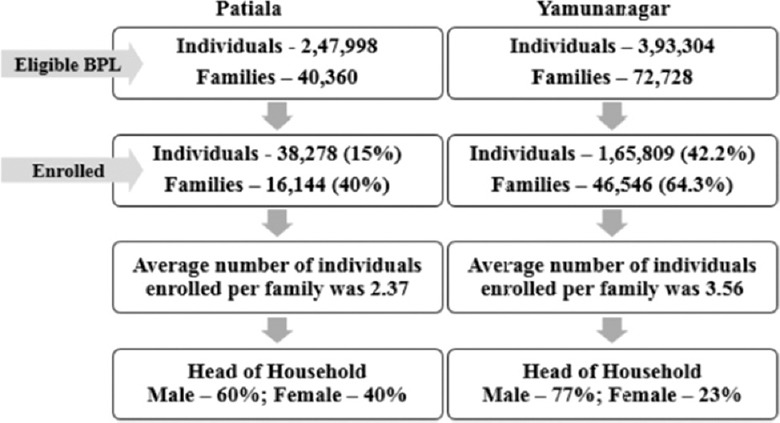
Insurance companies had considerable implementation responsibilities which led to conflict of interest in enrolment and empanelment. Enrolment was 15 per cent in Patiala and 42 per cent in Yamunanagar. Empanelment of health facilities was 17 (15%) in Patiala and 37 (30%) in Yamunanagar. Private-empanelled facilities were geographically clustered in the urban parts of the sub-districts. Monitoring was weak and led to breach of contracts. RSBY beneficiaries incurred out-of-pocket (OOP) expenditures (₹5748); however, it was lower than that for non-RSBY (₹10667). The scheme had in-built incentives for Centre, State, insurance companies and health providers (both public and private). There were no incentives for health staff for additional RSBY activities.
INTERPRETATION & CONCLUSIONS: RSBY has in-built incentives for all stakeholders. Some of the gaps identified in the scheme design pertained to poor enrolment practices, distribution of roles and responsibilities, fixed package rates, weak monitoring and supervision, and incurring OOP expenditure.
鉴于印度于 2018 年推出了阿育王保健计划,因此 Rashtriya Swasthya Bima Yojna(RSBY)的分析变得相关。本研究的目的是检验 RSBY 的计划设计和激励结构。
本研究分别在旁遮普邦的帕蒂亚拉和哈里亚纳邦的亚穆纳讷格尔地区进行(2011-2013 年)。这项混合方法研究包括对关键文件的审查;对关键利益相关者进行 20 次深入访谈;在帕蒂亚拉的 12 家指定 RSBY 承保医院对 RSBY 和非 RSBY 受益人的 399 次退出访谈,以及对州节点机构和地区医疗官的二级数据库进行分析。
保险公司承担了相当大的实施责任,这导致了在登记和承保方面存在利益冲突。帕蒂亚拉的登记率为 15%,亚穆纳讷格尔的登记率为 42%。医疗设施的承保率在帕蒂亚拉为 17(15%),在亚穆纳讷格尔为 37(30%)。私营承保的医疗机构在分区的城市部分呈地理聚集。监测不力导致合同违约。RSBY 受益人为自付费用(₹5748);然而,这低于非 RSBY(₹10667)。该计划为中央、邦、保险公司和卫生提供者(包括公共和私人)提供了内在激励。没有为卫生工作人员提供额外 RSBY 活动的激励措施。
RSBY 为所有利益相关者提供了内在激励。计划设计中存在一些差距,涉及登记做法不佳、角色和责任分配、固定套餐费率、监测和监督不力以及自付费用。