Chitongo P B, Roberts L N, Yang L, Patel R K, Lyall R, Luxton R, Aylwin S J B, Arya R
Department of Haematological Medicine, King's Thrombosis Centre, King's College Hospital, London, United Kingdom.
Department of Endocrinology, King's College Hospital, London, United Kingdom.
TH Open. 2017 Dec 15;1(2):e146-e154. doi: 10.1055/s-0037-1608942. eCollection 2017 Jul.
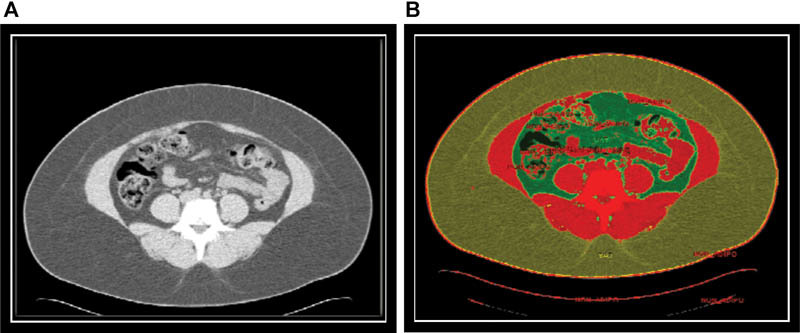
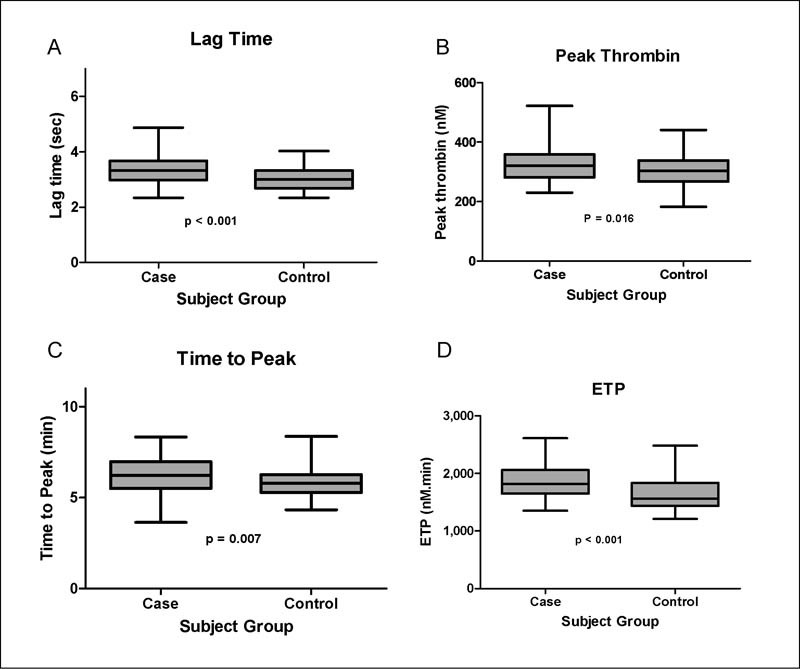
Increased visceral adipose tissue (VAT) has been shown to be associated with the development of insulin resistance, type 2 diabetes, stroke, and ischemic heart disease. It remains unknown whether fat distribution impacts on coagulation markers and/or the risk of venous thrombosis. This study evaluates markers of hypercoagulability in III obesity (body mass index [BMI] >40 kg/m ) compared with nonobese controls. We further investigated whether hypercoagulability was influenced by VAT, metabolic syndrome, and metabolic markers, including adiponectin. Ninety patients were recruited from the obesity clinic at King's College Hospital from November 2009 to December 2011. The inclusion criteria were class III obesity (BMI ≥40 kg/m ) and age 18 to 65 years. A control group (healthy ambulatory participants, with a BMI < 30 kg/m ) was recruited from volunteers responding to advertisement. Abdominal VAT and subcutaneous adipose tissue surface areas were determined by evaluation of a single-slice CT at spinal vertebra L4. Thrombin generation revealed a significantly increased peak and endogenous thrombin potential in patients compared with controls. Lag time and time to peak (ttP) were also significantly prolonged in patients. VAT was found to have the strongest association with thrombin generation parameters: lag time (β = 0.378; < 0.001), peak thrombin (0.378; = 0.04), and ttP (β = 0.373; = 0.001). BMI was found to be a predictor for lag time only (β = 0.313; = 0.003). SAT was not associated with any of the thrombin generation parameters (data not shown). VAT was found to be an independent determinant of peak thrombin, lag time, and ttP. The study suggests not only fat mass but also fat distribution, particularly visceral adiposity, mediates hypercoagulability in obesity.
内脏脂肪组织(VAT)增加已被证明与胰岛素抵抗、2型糖尿病、中风和缺血性心脏病的发生有关。脂肪分布是否会影响凝血标志物和/或静脉血栓形成的风险仍不清楚。本研究评估了III级肥胖(体重指数[BMI]>40kg/m²)患者与非肥胖对照组相比的高凝状态标志物。我们进一步研究了高凝状态是否受VAT、代谢综合征和包括脂联素在内的代谢标志物的影响。
2009年11月至2011年12月,从国王学院医院肥胖门诊招募了90名患者。纳入标准为III级肥胖(BMI≥40kg/m²)且年龄在18至65岁之间。对照组(健康门诊参与者,BMI<30kg/m²)从回应广告的志愿者中招募。通过评估第4腰椎的单层CT确定腹部VAT和皮下脂肪组织表面积。
与对照组相比,患者的凝血酶生成显示峰值和内源性凝血酶潜力显著增加。患者的延迟时间和达到峰值的时间(ttP)也显著延长。发现VAT与凝血酶生成参数的相关性最强:延迟时间(β=0.378;P<0.001)、凝血酶峰值(0.378;P=0.04)和ttP(β=0.373;P=0.001)。发现BMI仅是延迟时间的预测因子(β=0.313;P=0.003)。皮下脂肪组织(SAT)与任何凝血酶生成参数均无相关性(数据未显示)。发现VAT是凝血酶峰值、延迟时间和ttP的独立决定因素。该研究表明,不仅脂肪量,而且脂肪分布,特别是内脏脂肪过多,在肥胖中介导高凝状态。