NIHR Manchester Musculoskeletal Biomedical Research Centre, Central Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom.
Arthritis Research UK Centre for Epidemiology, Centre for Musculoskeletal Research, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, United Kingdom.
JMIR Mhealth Uhealth. 2019 Jul 2;7(7):e12952. doi: 10.2196/12952.
In contrast to the use of traditional unidimensional paper-based scales, a mobile health (mHealth) assessment of pain in children and young people (CYP) with juvenile idiopathic arthritis (JIA) enables comprehensive and complex multidimensional pain data to be captured remotely by individuals. However, how professionals use multidimensional pain data to interpret and synthesize pain reports gathered using mHealth tools is not yet known.
The aim of this study was to explore the salience and prioritization of different mHealth pain features as interpreted by key stakeholders involved in research and management of pain in CYP with JIA.
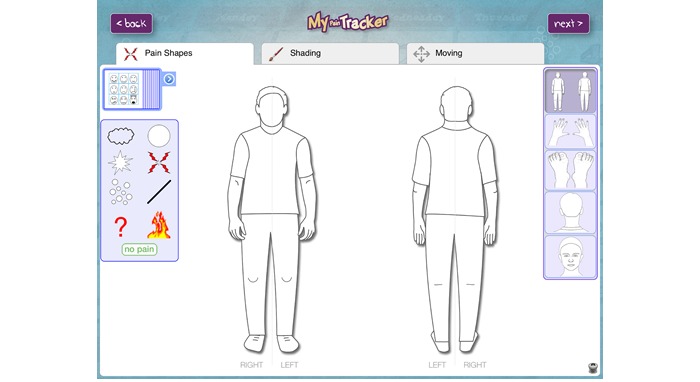
Pain and rheumatology specialists were purposively recruited via professional organizations. Face-to-face focus groups were conducted for each specialist group. Participants were asked to rank order 9 static vignette scenarios created from real patient mHealth multidimensional pain data. These data had been collected by a researcher in a separate study using My Pain Tracker, a valid and acceptable mHealth iPad pain communication tool that collects information about intensity, severity, location, emotion, and pictorial pain qualities. In the focus groups, specialists discussed their decision-making processes behind each rank order in the focus groups. The total group rank ordering of vignette scenarios was calculated. Qualitative data from discussions were analyzed using latent thematic analysis.
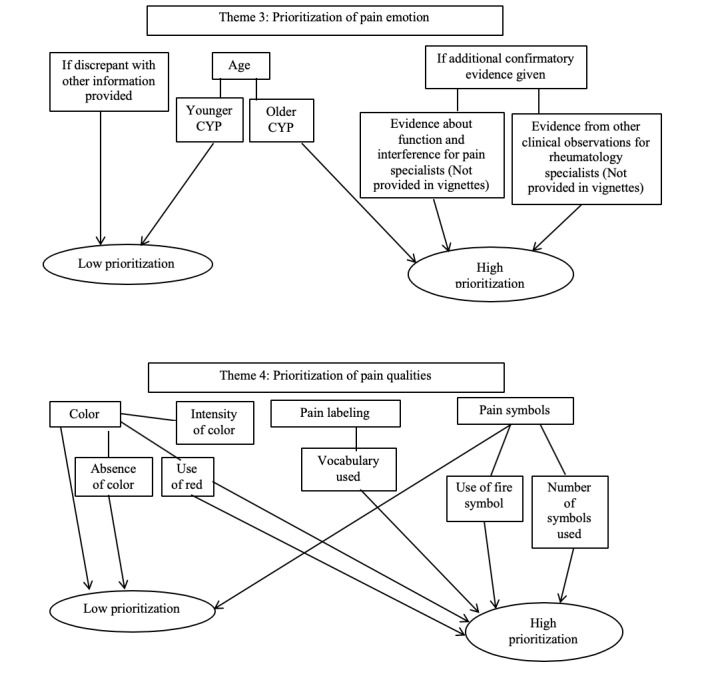
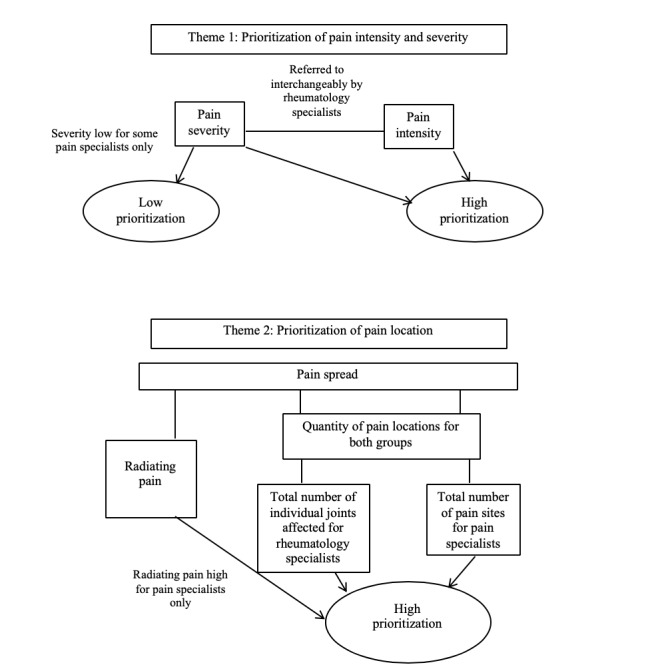
A total of 9 pain specialists took part in 1 focus group and 10 rheumatology specialists in another. In pain specialists, the consensus for the highest pain experience (44%) was poorer than their ranking of the lowest pain experiences (55%). Conversely, in rheumatology specialists, the consensus for the highest pain experience (70%) was stronger than their ranking of the lowest pain experience (50%). Pain intensity was a high priority for pain specialists, but rheumatology specialists gave high priority to intensity and severity taken together. Pain spread was highly prioritized, with the number of pain locations (particular areas or joints) being a high priority for both groups; radiating pain was a high priority for pain specialists only. Pain emotion was challenging for both groups and was only perceived to be a high priority when specialists had additional confirmatory evidence (such as information about pain interference or clinical observations) to validate the pain emotion report. Pain qualities such as particular word descriptors, use of the color red, and fire symbols were seen to be high priority by both groups in interpretation of CYP pain reports.
Pain interpretation is complex. Findings from this study of specialists' decision-making processes indicate which aspects of pain are prioritized and weighted more heavily than others by those interpreting mHealth data. Findings are useful for developing electronic graphical summaries which assist specialists in interpreting patient-reported mHealth pain data more efficiently in clinical and research settings.
与传统的一维纸质量表的使用相比,移动医疗(mHealth)可远程对儿童和青少年(CYP)的疼痛进行全面、复杂的多维评估,由个体采集疼痛数据。然而,专业人员如何使用多维疼痛数据来解释和综合使用 mHealth 工具收集的疼痛报告还不得而知。
本研究旨在探讨参与儿童和青少年幼年特发性关节炎(JIA)疼痛研究和管理的关键利益相关者如何解释 mHealth 疼痛特征的重要性和优先级。
通过专业组织有针对性地招募疼痛和风湿病专家。为每个专家小组进行面对面的焦点小组讨论。要求参与者对 9 个静态情景案例进行排序,这些案例是从使用 My Pain Tracker 的真实患者 mHealth 多维疼痛数据中创建的。该研究使用 My Pain Tracker 收集有关强度、严重程度、位置、情绪和图像疼痛质量的信息,这是一种有效的、可接受的 mHealth iPad 疼痛交流工具,该工具已由一名研究人员在单独的研究中收集。在焦点小组中,专家们讨论了他们在每个焦点小组中进行排序的决策过程。计算了情景案例的总组排序。使用潜在主题分析对讨论中的定性数据进行分析。
共有 9 名疼痛专家参加了 1 个焦点小组,10 名风湿病专家参加了另一个焦点小组。在疼痛专家中,对最高疼痛体验(44%)的共识低于对最低疼痛体验(55%)的共识。相反,在风湿病专家中,对最高疼痛体验(70%)的共识高于对最低疼痛体验(50%)的共识。疼痛强度是疼痛专家的首要任务,但风湿病专家更重视强度和严重程度相结合。疼痛扩散受到高度重视,疼痛部位的数量(特定区域或关节)是两组的高度优先事项;放射痛是疼痛专家的高度优先事项。情绪疼痛对两组来说都是一个挑战,只有当专家有额外的确认性证据(例如关于疼痛干扰或临床观察的信息)来验证疼痛情绪报告时,他们才会认为疼痛情绪是一个高度优先事项。两组都认为疼痛质量(如特定的单词描述、使用红色和火焰符号)是解释 CYP 疼痛报告的高度优先事项。
疼痛解释是复杂的。本研究中对专家决策过程的研究结果表明,解释 mHealth 数据的人更重视疼痛的哪些方面,并对这些方面赋予更高的权重。研究结果对于开发电子图形摘要很有用,这些摘要有助于专家在临床和研究环境中更有效地解释患者报告的 mHealth 疼痛数据。