Stefan Gabriel, Stancu Simona, Zugravu Adrian, Petre Nicoleta, Mandache Eugen, Mircescu Gabriel
Dr Carol Davila Teaching Hospital of Nephrology, University of Medicine and Pharmacy Carol Davila.
Dr Carol Davila Teaching Hospital of Nephrology, Bucharest, Romania.
Medicine (Baltimore). 2019 Jul;98(27):e16333. doi: 10.1097/MD.0000000000016333.
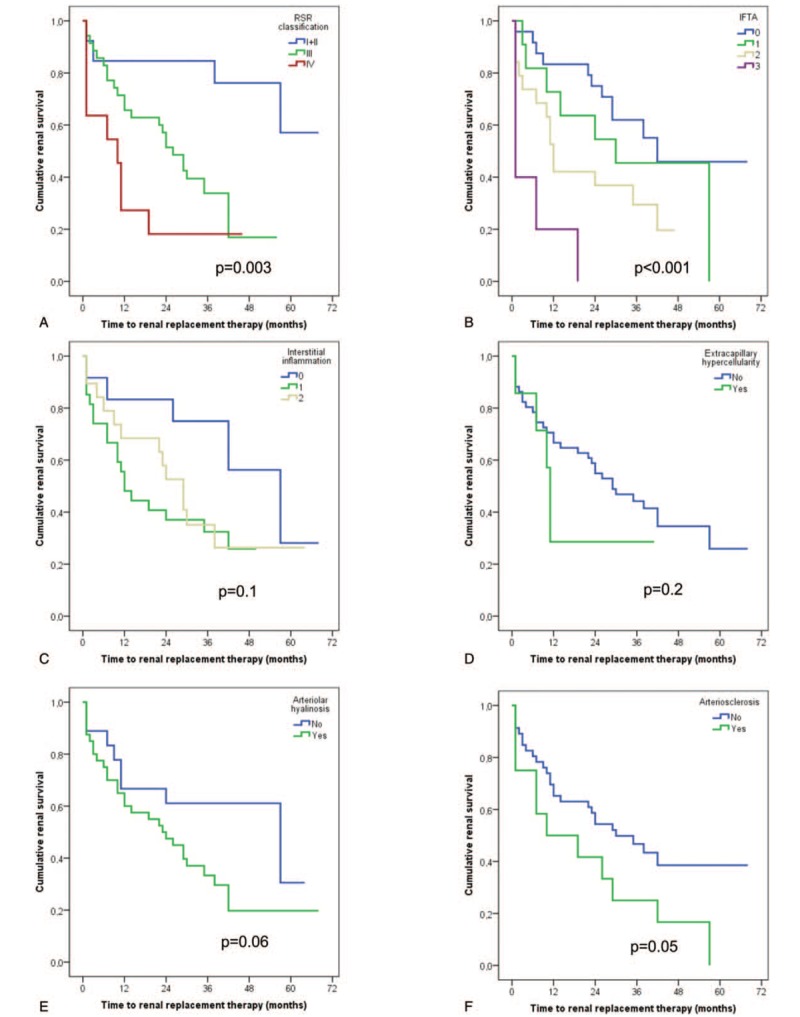
The prognostic utility of histologic features in patients with diabetic nephropathy (DN) classified according to the Renal Pathology Society (RPS) classification is controversial. Therefore, we aimed to evaluate the relationship between histologic changes and renal outcome in DN patients.We examined the renal outcome at November 30, 2017 of 74 adult patients (median age of 54.6 years, 69% male, 81% diabetes mellitus (DM) type 2, estimated GFR (eGFR) 29.6 mL/min) with biopsy proven DN between 2010 and 2015. The primary endpoint was renal replacement therapy (RRT) initiation.Half of the patients progressed to end stage renal disease (ESRD) during follow-up; they had lower eGFR, increased proteinuria, hematuria and serum cholesterol. Regarding the pathologic features, they were more frequently in class III and IV, had higher interstitial fibrosis and tubular atrophy score (IFTA), increased interstitial inflammation, more frequent arteriolar hyalinosis and higher glomerular basement membrane (GBM) thickness. The mean kidney survival time was 2.7 (95%CI 2.1, 3.3) years. In univariate time-dependent analyses, higher RPS DN class, increased IFTA, the presence of arteriolar hyalinosis and arteriosclerosis were associated with RRT initiation.In the fully adjusted model, the clinical characteristics associated with poor renal survival were longer duration of DM, lower eGFR, increased proteinuria and higher hematuria and the only pathologic lesions to remain significant were the GBM thickness and the IFTA.In conclusion, in this European cohort, the severity of glomerular lesions evaluated with the RPS DN classification had limited utility in predicting RRT initiation. However, IFTA and GBM thickness were significantly associated with renal survival.
根据肾脏病理学会(RPS)分类法分类的糖尿病肾病(DN)患者的组织学特征的预后效用存在争议。因此,我们旨在评估DN患者组织学变化与肾脏结局之间的关系。我们研究了2010年至2015年间74例经活检证实为DN的成年患者(中位年龄54.6岁,69%为男性,81%为2型糖尿病(DM),估计肾小球滤过率(eGFR)为29.6 mL/min)在2017年11月30日的肾脏结局。主要终点是开始肾脏替代治疗(RRT)。一半的患者在随访期间进展为终末期肾病(ESRD);他们的eGFR较低,蛋白尿、血尿和血清胆固醇增加。关于病理特征,他们更常处于III级和IV级,间质纤维化和肾小管萎缩评分(IFTA)更高,间质炎症增加,小动脉玻璃样变更频繁,肾小球基底膜(GBM)厚度更高。平均肾脏生存时间为2.7(95%CI 2.1, 3.3)年。在单变量时间依赖性分析中,较高的RPS DN分级、IFTA增加、小动脉玻璃样变和动脉硬化的存在与开始RRT相关。在完全调整模型中,与肾脏生存不良相关的临床特征是DM病程较长、eGFR较低、蛋白尿增加、血尿较高,唯一仍具有显著意义的病理病变是GBM厚度和IFTA。总之,在这个欧洲队列中,用RPS DN分类法评估的肾小球病变严重程度在预测RRT开始方面的效用有限。然而,IFTA和GBM厚度与肾脏生存显著相关。