Fraioli Francesco, Lyasheva Maria, Porter Joanna C, Bomanji Jamshed, Shortman Robert I, Endozo Raymond, Wan Simon, Bertoletti Linda, Machado Maria, Ganeshan Balaji, Win Thida, Groves Ashley M
Institute of Nuclear Medicine, UCL(H) and University College London Hospital, 235 Euston Rd, London, NW1 2BU, UK.
Department of Oncology, School of Clinical Medicine, University of Cambridge, Cambridge, UK.
Eur J Nucl Med Mol Imaging. 2019 Sep;46(10):2023-2031. doi: 10.1007/s00259-019-04386-5. Epub 2019 Jul 8.
To investigate the combined performance of quantitative CT (qCT) following a computer algorithm analysis (IMBIO) and F-FDG PET/CT to assess survival in patients with idiopathic pulmonary fibrosis (IPF).
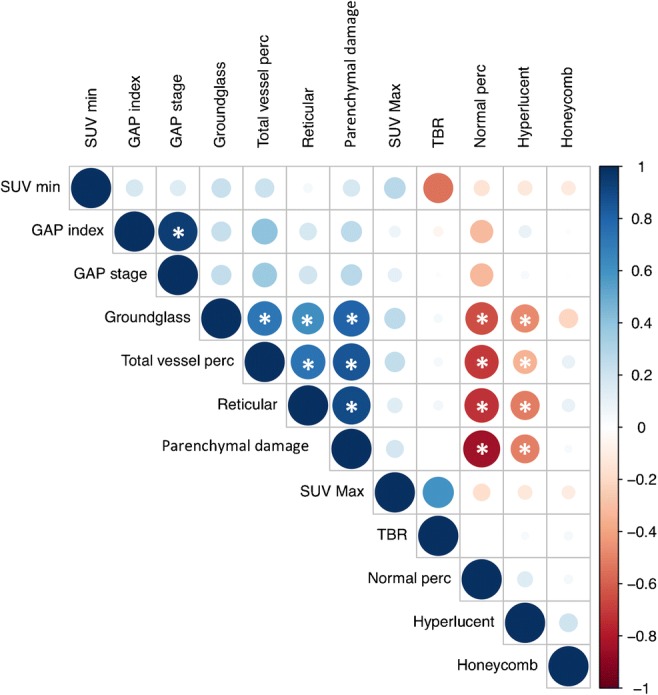
A total of 113 IPF patients (age 70 ± 9 years) prospectively and consecutively underwent F-FDG PET/CT and high-resolution CT (HRCT) at our institution. During a mean follow-up of 29.6 ± 26 months, 44 (48%) patients died. As part of the qCT analysis, pattern evaluation of HRCT (using IMBIO software) included the total extent (percentage) of the following features: normal-appearing lung, hyperlucent lung, parenchymal damage (comprising ground-glass opacification, reticular pattern and honeycombing), and the pulmonary vessels. The maximum (SUV) and minimum (SUV) standardized uptake value (SUV) for F-FDG uptake in the lungs, and the target-to-background (SUV/SUV) ratio (TBR) were quantified using routine region-of-interest (ROI) analysis. Pulmonary functional tests (PFTs) were acquired within 14 days of the PET/CT/HRCT scan. Kaplan-Meier (KM) survival analysis was used to identify associations with mortality.
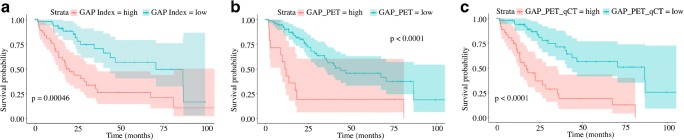
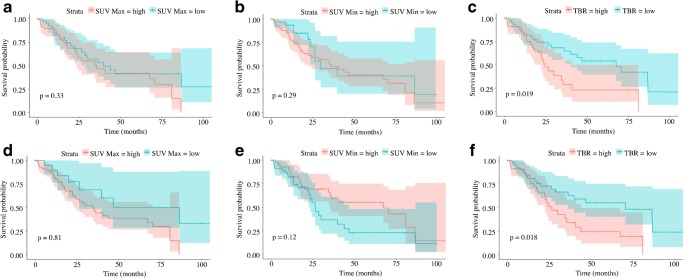
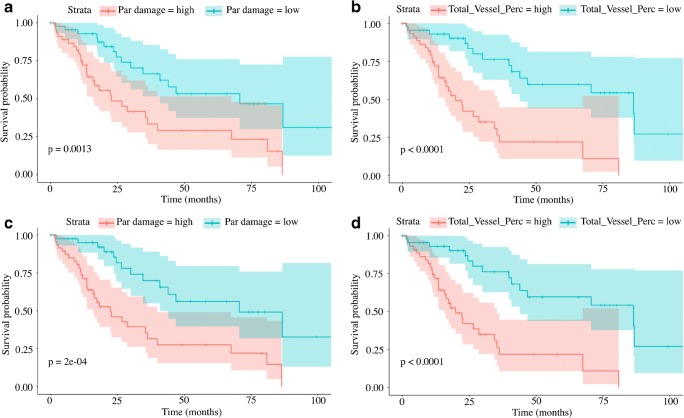
Data from 91 patients were available for comparative analysis. The average ± SD GAP [gender, age, physiology] score was 4.2 ± 1.7 (range 0-8). The average ± SD SUV, SUV, and TBR were 3.4 ± 1.4, 0.7 ± 0.2, and 5.6 ± 2.8, respectively. In all patients, qCT analysis demonstrated a predominantly reticular lung pattern (14.9 ± 12.4%). KM analysis showed that TBR (p = 0.018) and parenchymal damage assessed by qCT (p = 0.0002) were the best predictors of survival. Adding TBR and qCT to the GAP score significantly increased the ability to differentiate between high and low risk (p < 0.0001).
F-FDG PET and qCT are independent and synergistic in predicting mortality in patients with IPF.
研究定量CT(qCT)结合计算机算法分析(IMBIO)和F-FDG PET/CT评估特发性肺纤维化(IPF)患者生存率的联合性能。
共有113例IPF患者(年龄70±9岁)在我院前瞻性、连续地接受了F-FDG PET/CT和高分辨率CT(HRCT)检查。在平均29.6±26个月的随访期间,44例(48%)患者死亡。作为qCT分析的一部分,HRCT的模式评估(使用IMBIO软件)包括以下特征的总范围(百分比):外观正常的肺、肺透亮度增加、实质损害(包括磨玻璃影、网状影和蜂窝状影)以及肺血管。使用常规感兴趣区(ROI)分析对肺内F-FDG摄取的最大(SUV)和最小(SUV)标准化摄取值(SUV)以及靶本比(SUV/SUV)(TBR)进行量化。在PET/CT/HRCT扫描后14天内进行肺功能测试(PFT)。采用Kaplan-Meier(KM)生存分析来确定与死亡率的关联。
91例患者的数据可用于比较分析。平均±标准差GAP[性别、年龄、生理学]评分为4.2±1.7(范围0-8)。平均±标准差SUV、SUV和TBR分别为3.4±1.4、0.7±0.2和5.6±2.8。在所有患者中,qCT分析显示主要为网状肺模式(14.9±12.4%)。KM分析表明,TBR(p=0.018)和qCT评估的实质损害(p=0.0002)是生存的最佳预测指标。将TBR和qCT添加到GAP评分中显著提高了区分高风险和低风险的能力(p<0.0001)。
F-FDG PET和qCT在预测IPF患者死亡率方面具有独立性和协同性。