Heart Disease Prevention Program, Division of Cardiology, C240 Medical Sciences, University of California, Irvine, Irvine, CA, 92697, USA.
Division of Cardiovascular Medicine, University of California, Davis, Davis, USA.
Am J Cardiovasc Drugs. 2020 Feb;20(1):1-9. doi: 10.1007/s40256-019-00358-0.
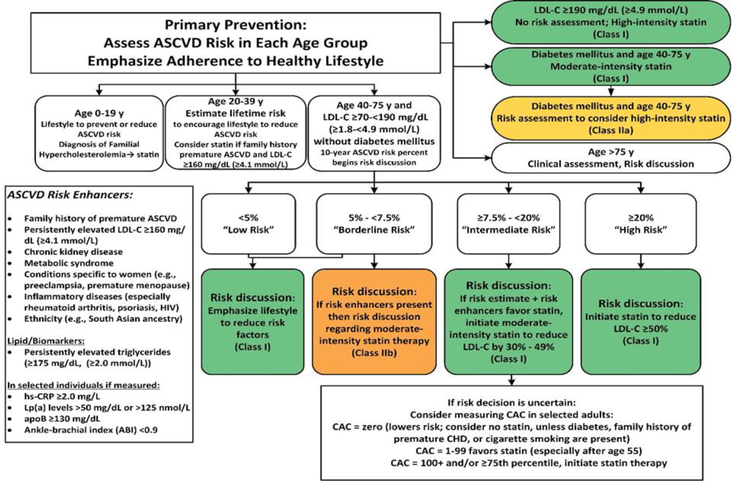
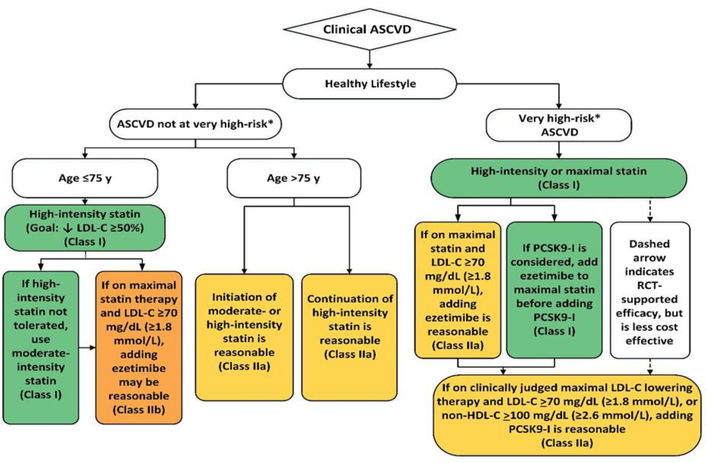
The 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol retains focus on recommendations for statin treatment in the original four statin-eligible groups [those with atherosclerotic cardiovascular disease (ASCVD), diabetes, low-density lipoprotein cholesterol (LDL-C) ≥ 190 mg/dL, and higher risk primary prevention] without the use of treatment initiation or target LDL-C levels from the earlier 2013 American College of Cardiology/American Heart Association (ACC/AHA) guideline, but has several new features. First, patients with primary prevention are divided into those who are at low (< 5%), borderline (5% to < 7.5%), intermediate (7.5% to < 20%), and high (≥ 20%) risk based on the ASCVD risk estimator. Moreover, the new guideline goes further to consider a wider range of factors [now called "risk enhancers"-premature family history of ASCVD, persistently high LDL-C, chronic kidney disease (CKD), metabolic syndrome, conditions specific to women, inflammatory diseases, and high-risk ethnicities] that can be used to better inform the treatment decision. Moreover, more detailed recommendations on how the results of coronary calcium scanning can be used to inform the treatment decision are provided, including how it may be used to "de-risk" certain patients for delaying or avoiding the use of statin therapy. There are also specific sections for cholesterol management in other patient subgroups including women, children, certain ethnic groups, those with CKD, chronic inflammatory disorders and HIV, as well as discussion on the management of hypertriglyceridemia. Importantly, for persons with known ASCVD, a distinction is made for those who are at "very high risk" based on having had two major ASCVD events or one major event and two or more other high risk conditions, such as diabetes or other major risk factors, or bypass surgery or percutaneous intervention. Finally, the concept of a threshold LDL-C for initiating a non-statin therapy (after considering highest tolerated statin dosage) is provided, with ezetimibe recommended as the key non-statin to be added if the LDL-C still remains ≥ 70 mg/dL for all ASCVD patients, and in those who are at "very high risk", further consideration for using a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor. While the new guideline does have greater detail (and arguably, complexity), the refinements provide a strategy for guiding the clinician to target both statin and non-statin therapy to those most likely to derive benefit.
2018 年美国心脏协会(AHA)/美国心脏病学会(ACC)/美国心血管血管造影和介入学会(AACVPR)/美国医师协会(AAPA)/美国临床内分泌医师协会(ABC)/美国医师协会(ACPM)/美国糖尿病协会(ADA)/美国老年医学会(AGS)/美国药学会(APhA)/美国临床病理学会(ASPC)/北美绝经协会(NLA)/美国医师学院(PCNA)联合发布的《成人降胆固醇治疗指南》保留了他汀类药物治疗在原始四个他汀类药物适应证组(动脉粥样硬化性心血管疾病(ASCVD)、糖尿病、低密度脂蛋白胆固醇(LDL-C)≥190mg/dL 和更高风险的一级预防)中的建议,而不使用更早的 2013 年美国心脏病学会/美国心脏协会(ACC/AHA)指南中的起始治疗或 LDL-C 目标值,但有几个新特点。首先,根据 ASCVD 风险估计器,将一级预防患者分为低危(<5%)、中危(5%至<7.5%)、高危(7.5%至<20%)和极高危(≥20%)。此外,新指南进一步考虑了更广泛的因素[现在称为“风险增强剂”-早发性 ASCVD 家族史、持续高 LDL-C、慢性肾脏病(CKD)、代谢综合征、女性特有的疾病、炎症性疾病和高危种族],以更好地为治疗决策提供信息。此外,还提供了关于如何使用冠状动脉钙扫描结果来告知治疗决策的更详细建议,包括如何将其用于“降低风险”某些患者,以延迟或避免使用他汀类药物治疗。对于包括女性、儿童、某些种族、CKD、慢性炎症性疾病和 HIV 患者在内的其他患者亚组的胆固醇管理也有专门的章节,以及对高甘油三酯血症的管理进行讨论。重要的是,对于已知有 ASCVD 的患者,根据是否发生过两次重大 ASCVD 事件或一次重大事件和两次或更多其他高危情况(如糖尿病或其他高危因素、旁路手术或经皮介入),对那些处于“极高危”的患者进行区分。最后,提供了启动非他汀类药物治疗的 LDL-C 阈值(在考虑最高耐受他汀类药物剂量后)的概念,如果所有 ASCVD 患者的 LDL-C 仍≥70mg/dL,或在“极高危”患者中,如果 LDL-C 仍≥70mg/dL,建议使用依折麦布作为关键的非他汀类药物,如果 LDL-C 仍≥70mg/dL,进一步考虑使用前蛋白转化酶枯草溶菌素 9(PCSK9)抑制剂。虽然新指南确实有更详细的信息(可以说也更复杂),但这些细化为指导临床医生将他汀类药物和非他汀类药物治疗靶向最有可能获益的患者提供了一种策略。