Center for Surgery and Public Health, Department of Surgery, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
Center for Surgery and Public Health, Division of Urology, Department of Surgery, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2019 Jul 3;2(7):e196673. doi: 10.1001/jamanetworkopen.2019.6673.
The increased use of prescription opioid medications has contributed to an epidemic of sustained opioid use, misuse, and addiction. Adults of working age are thought to be at greatest risk for prescription opioid dependence.
To develop a risk score (the Stopping Opioids After Surgery score) for sustained prescription opioid use after surgery in a working-age population using readily available clinical information.
DESIGN, SETTING, AND PARTICIPANTS: In this case-control study, claims from TRICARE (the insurance program of the US Department of Defense) for working-age adult (age 18-64 years) patients undergoing 1 of 10 common surgical procedures from October 1, 2005, to September 30, 2014, were queried. A logistic regression model was used to identify variables associated with sustained prescription opioid use. The point estimate for each variable in the risk score was determined by its β coefficient in the model. The risk score for each patient represented the summed point totals, ranging from 0 to 100, with a lower score indicating lower risk of sustained prescription opioid use. Data were analyzed from September 25, 2018, to February 5, 2019.
Exposures were age; race; sex; marital status; socioeconomic status; discharge disposition; procedure intensity; length of stay; intensive care unit admission; comorbid diabetes, liver disease, renal disease, malignancy, depression, or anxiety; and prior opioid use status.
The primary outcome was sustained prescription opioid use, defined as uninterrupted use for 6 months following surgery. A risk score for each patient was calculated and then used as a predictor of sustained opioid use after surgical intervention. The area under the curve and the Brier score were used to determine the accuracy of the scoring system and the Hosmer-Lemeshow goodness-of-fit test was used to evaluate model calibration.
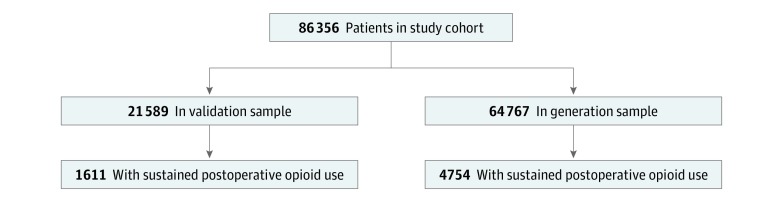
Of 86 356 patients in the analysis (48 827 [56.5%] male; mean [SD] age, 46.5 [14.5] years), 6365 (7.4%) met criteria for sustained prescription opioid use. The sample used for model generation consisted of 64 767 patients, while the validation sample had 21 589 patients. Prior opioid exposure was the factor most strongly associated with sustained opioid use (odds ratio, 13.00; 95% CI, 11.87-14.23). The group with the lowest scores (<31) had a mean (SD) 4.1% (2.5%) risk of sustained opioid use; those with intermediate scores (31-50) had a mean (SD) risk of 14.9% (6.3%); and those with the highest scores (>50) had a mean (SD) risk of 35.8% (3.6%).
This study developed an intuitive and accessible opioid risk assessment applicable to the care of working-age patients following surgery. This tool is scalable to clinical practice and can potentially be incorporated into electronic medical record platforms to enable automated calculation and clinical alerts that are generated in real time.
处方类阿片类药物使用的增加导致了持续使用阿片类药物、滥用和成瘾的流行。处于工作年龄的成年人被认为是处方类阿片类药物依赖的最大风险人群。
利用易于获得的临床信息,为工作年龄人群在手术后持续使用处方类阿片类药物开发一个风险评分(术后手术持续使用阿片类药物评分)。
设计、地点和参与者:在这项病例对照研究中,查询了 2005 年 10 月 1 日至 2014 年 9 月 30 日期间接受 10 项常见手术之一的美国国防部医疗保险计划(TRICARE)的工作年龄(18-64 岁)成年患者的索赔信息。使用逻辑回归模型确定与持续使用处方类阿片类药物相关的变量。风险评分中每个变量的点估计值由其在模型中的β系数确定。每个患者的风险评分代表总积分,范围为 0 到 100,得分越低表示持续使用处方类阿片类药物的风险越低。数据分析于 2018 年 9 月 25 日至 2019 年 2 月 5 日进行。
年龄;种族;性别;婚姻状况;社会经济地位;出院情况;手术强度;住院时间;入住重症监护病房;合并糖尿病、肝脏疾病、肾脏疾病、恶性肿瘤、抑郁或焦虑;以及先前使用阿片类药物的情况。
主要结果是持续使用处方类阿片类药物,定义为手术后 6 个月内不间断使用。为每位患者计算了一个风险评分,并将其用作手术干预后持续使用阿片类药物的预测因子。曲线下面积和 Brier 评分用于确定评分系统的准确性,Hosmer-Lemeshow 拟合优度检验用于评估模型校准。
在分析中,86356 名患者(48827[56.5%]名男性;平均[SD]年龄,46.5[14.5]岁)中,有 6365 名(7.4%)符合持续使用处方类阿片类药物的标准。用于模型生成的样本包括 64767 名患者,而验证样本有 21589 名患者。先前使用阿片类药物是与持续使用阿片类药物最密切相关的因素(比值比,13.00;95%CI,11.87-14.23)。分数最低(<31)的组持续使用阿片类药物的平均(SD)风险为 4.1%(2.5%);分数中等(31-50)的组平均(SD)风险为 14.9%(6.3%);分数最高(>50)的组平均(SD)风险为 35.8%(3.6%)。
这项研究开发了一种直观且易于使用的阿片类药物风险评估方法,适用于手术后工作年龄患者的护理。该工具可扩展到临床实践中,并可潜在地整合到电子病历平台中,以实现实时自动计算和临床警报。