Division of Pediatric Cardiology, Department of Pediatrics, Leiden University Medical Center, Leiden, The Netherlands.
Department of Cardiology, Amsterdam UMC, Univ of Amsterdam, Amsterdam, The Netherlands.
Heart. 2019 Nov;105(22):1732-1740. doi: 10.1136/heartjnl-2019-315157. Epub 2019 Jul 10.
To study neo-aortic growth and the evolution of neo-aortic valve regurgitation (AR) in patients with transposition of the great arteries (TGA) after arterial switch operation (ASO) from newborn to adulthood and to identify patients at risk.
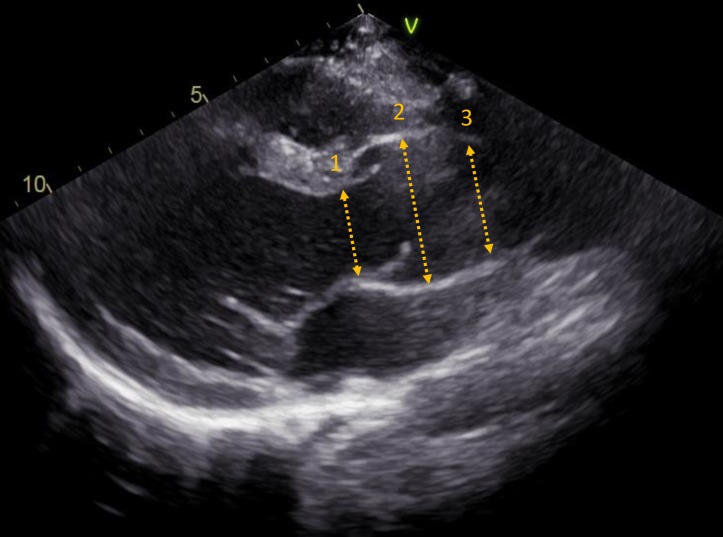
Neo-aortic dimensions (annulus/root/sinotubular junction) and neo-aortic valve regurgitation were assessed serially in 345 patients with TGA who underwent ASO between 1977 and 2015. Linear mixed-effect models were used to assess increase of neo-aortic dimensions over time and to identify risk factors for dilatation. Risk factor analysis for AR by using time-dependent Cox regression models.
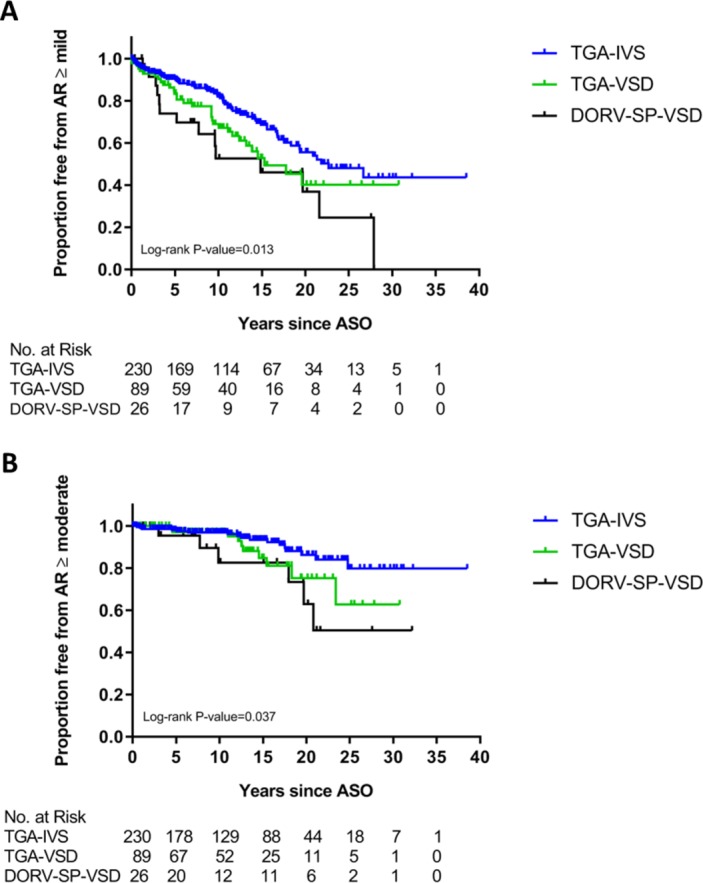
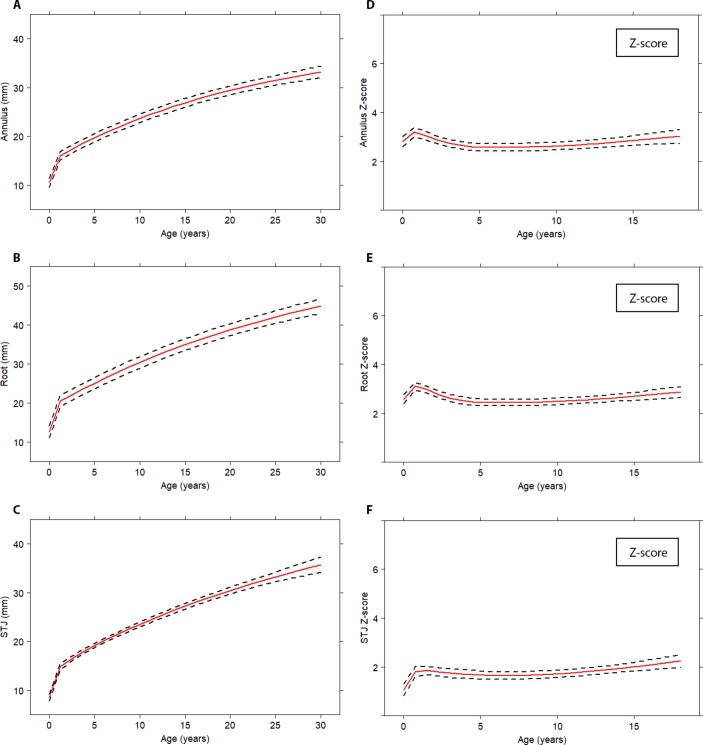
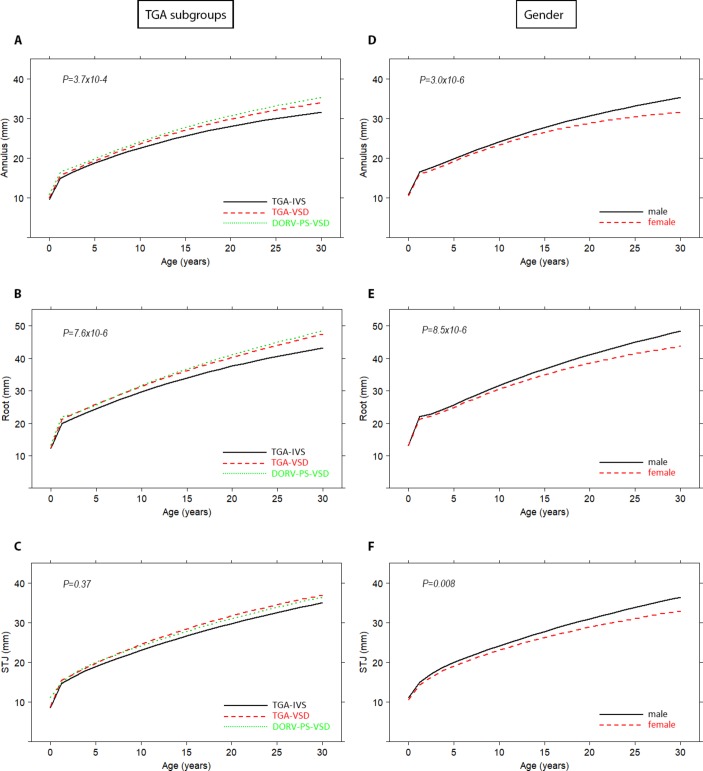
After a rapid increase in the first year after ASO and proportional growth in childhood, neo-aortic dimensions continue to increase in adulthood without stabilisation. Annual diameter increase in adulthood was 0.39±0.06, 0.63±0.09 and 0.54±0.11 mm for, respectively, neo-aortic annulus, root and sinotubular junction, all significantly exceeding normal growth. AR continues to develop over time: freedom from AR ≥moderate during the first 25 years post-ASO was 69%. Risk factors for root dilatation were complex TGA anatomy (TGA-ventricular septal defect (VSD), double outlet right ventricle with subpulmonary VSD) and male gender. Risk factors for AR ≥moderate were: complex TGA anatomy and neo-aortic growth. Per millimetre increase in aortic root dimension, there was a 9% increase in the hazard of AR ≥moderate. Bicuspid pulmonary valve did not relate to the presence of root dilatation or AR.
After ASO, neo-aortic dilatation proceeds beyond childhood and is associated with an increase in AR incidence over time. Careful follow-up of the neo-aortic valve and root function is mandatory, especially in males and in patients with complex TGA anatomy.
研究大动脉转位(TGA)患者经动脉调转术(ASO)后从新生儿到成年的升主动脉(neo-aorta)生长和 neo-aortic 瓣反流(AR)的演变,并确定高危患者。
对 1977 年至 2015 年间接受 ASO 的 345 例 TGA 患者进行了 neo-aortic 尺寸(瓣环/根部/窦管交界处)和 neo-aortic 瓣反流的系列评估。使用线性混合效应模型评估 neo-aortic 尺寸随时间的增加,并确定扩张的危险因素。使用时依 Cox 回归模型对 AR 进行危险因素分析。
ASO 后第一年 neo-aortic 快速增长,儿童期呈比例生长,成年后仍持续增长而无稳定期。成年后 neo-aortic 直径每年分别增加 0.39±0.06、0.63±0.09 和 0.54±0.11mm,均显著超过正常生长。AR 随时间继续发展:ASO 后 25 年内 AR 无中度或重度的比例为 69%。根部扩张的危险因素包括复杂的 TGA 解剖结构(TGA-室间隔缺损(VSD)、右心室双出口伴肺动脉瓣下 VSD)和男性。中度或重度 AR 的危险因素为:复杂的 TGA 解剖结构和 neo-aortic 生长。主动脉根部尺寸每增加 1 毫米,AR 中度或重度的危险比增加 9%。二叶式肺动脉瓣与根部扩张或 AR 无关。
ASO 后,neo-aortic 扩张超过儿童期,并随时间推移 AR 发生率增加。必须对 neo-aortic 瓣和根部功能进行仔细随访,尤其是在男性和复杂 TGA 解剖结构的患者中。