Akpede George O, Asogun Danny A, Okogbenin Sylvanus A, Dawodu Simeon O, Momoh Mojeed O, Dongo Andrew E, Ike Chiedozie, Tobin Ekaete, Akpede Nosa, Ogbaini-Emovon Ephraim, Adewale Adetunji E, Ochei Oboratare, Onyeke Frank, Okonofua Martha O, Atafo Rebecca O, Odia Ikponmwosa, Adomeh Donatus I, Odigie George, Ogbeifun Caroline, Muebonam Ekene, Ihekweazu Chikwe, Ramharter Michael, Colubri Andres, Sarbeti Pardis C, Happi Christian T, Günther Stephan, Agbonlahor Dennis E
Institute of Lassa Fever Research and Control, Irrua Specialist Teaching Hospital, Irrua, Nigeria.
Department of Paediatrics, Irrua Specialist Teaching Hospital, Irrua, Nigeria.
Front Public Health. 2019 Jun 25;7:170. doi: 10.3389/fpubh.2019.00170. eCollection 2019.
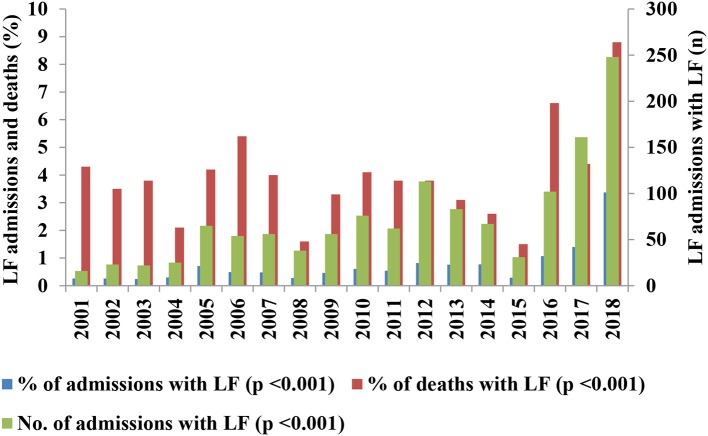
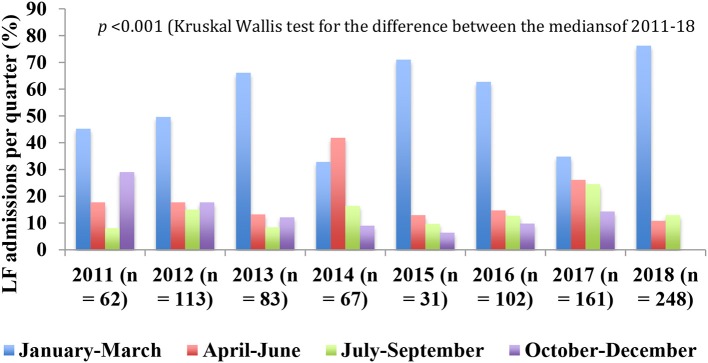
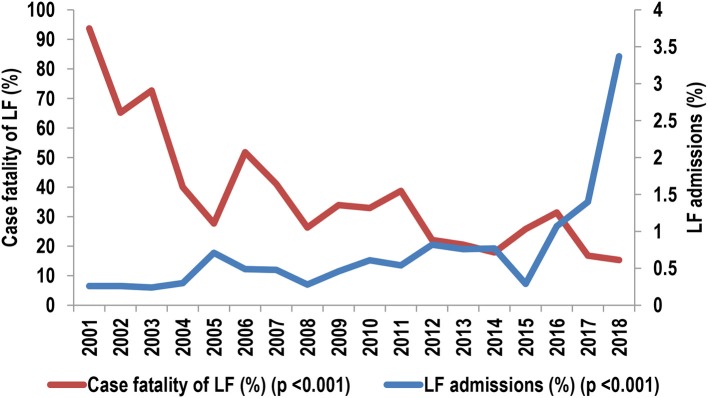
The general lack of comprehensive data on the trends of Lassa fever (LF) outbreaks contrasts with its widespread occurrence in West Africa and is an important constraint in the design of effective control measures. We reviewed the contribution of LF to admissions and mortality among hospitalized patients from 2001 to 2018 in the bid to address this gap. Observational study of LF caseload and mortality from 2001 to 18 in terms of the contribution of confirmed LF to admissions and deaths, and case fatality (CF) among patients with confirmed LF at a specialist center in Nigeria. The diagnosis of LF was confirmed using reverse transcription polymerase chain reaction (RT-PCR) test, and medians and frequencies were compared using Kruskal-Wallis, Mann-Whitney and χ2 tests, with -values <0.05 taken as significant. The contribution of confirmed LF to deaths (362/9057, 4.0%) was significantly higher than to admissions (1,298/185,707, 0.7%; OR [95% CI] = 5.9 [5.3, 6.7], < 0.001). The average CF among patients with confirmed LF declined from 154/355 (43%) in 2001-09 to 183/867 (21.1%) (OR [95% CI] = 2.9 [2.2, 3.7], < 0.001) in 2011-18. The annual CF declined from 94% in 2001 to 15% in 2018 whereas the caseload increased from 0.3 to 3.4%. The outbreaks were characterized by irregular cycles of high caseload in 2005-2007, 2012-2014, and 2016-2018, and progressive blurring of the seasonality. LF outbreaks in Nigeria have upgraded spatially and temporally, with the potential for cycles of increasing severity. The strategic establishment of LF surveillance and clinical case management centers could be a pragmatic and cost-effective approach to mitigating the outbreaks, particularly in reducing the associated CF. Urgent efforts are needed in reinvigorating extant control measures while the search for sustainable solutions continues.
拉沙热(LF)疫情趋势方面普遍缺乏全面数据,这与其在西非广泛传播的情况形成反差,也是设计有效控制措施的一个重要制约因素。为填补这一空白,我们回顾了2001年至2018年期间拉沙热对住院患者入院率和死亡率的影响。对2001年至2018年期间拉沙热病例数和死亡率进行观察性研究,内容包括确诊的拉沙热对入院和死亡的影响,以及尼日利亚一家专科中心确诊拉沙热患者的病死率(CF)。使用逆转录聚合酶链反应(RT-PCR)检测确诊拉沙热,采用Kruskal-Wallis、Mann-Whitney和χ2检验比较中位数和频率,P值<0.05为有统计学意义。确诊的拉沙热对死亡的影响(362/9057,4.0%)显著高于对入院的影响(1298/185707,0.7%;比值比[95%置信区间]=5.9[5.3,6.7],P<0.001)。确诊拉沙热患者的平均病死率从2001 - 2009年的154/355(43%)降至2011 - 2018年的183/867(21.1%)(比值比[95%置信区间]=2.9[2.2,3.7],P<0.001)。年病死率从2001年的94%降至2018年的15%,而病例数从0.3%增至3.4%。疫情的特点是在2005 - 2007年、2012 - 2014年和2016 - 2018年出现病例数高的不规则周期,且季节性逐渐模糊。尼日利亚的拉沙热疫情在空间和时间上都有升级,有严重程度增加的周期趋势。战略性地建立拉沙热监测和临床病例管理中心可能是减轻疫情,特别是降低相关病死率的一种务实且具成本效益的方法。在继续寻找可持续解决方案的同时,迫切需要努力重振现有的控制措施。