Parker Colleen H, Tomlinson George, Correia Adriano, Liu Louis W C
Division of Gastroenterology, Department of Medicine, University of Toronto, Toronto, Ontario, Canada.
Department of Medicine, University Health Network, Toronto, Ontario, Canada.
J Can Assoc Gastroenterol. 2018 Mar 30;1(2):60-66. doi: 10.1093/jcag/gwy010. eCollection 2018 Jun.
Dyssynergic defecation (DD) is present in approximately 30% of patients with idiopathic chronic constipation (CC). Diagnostic criteria for DD require objective testing such as anorectal manometry (ARM); yet, ARM remains a limited resource in Canada. The aim of this study is to determine the predictability of DD in patients with CC using a standardized self-reported symptom questionnaire.
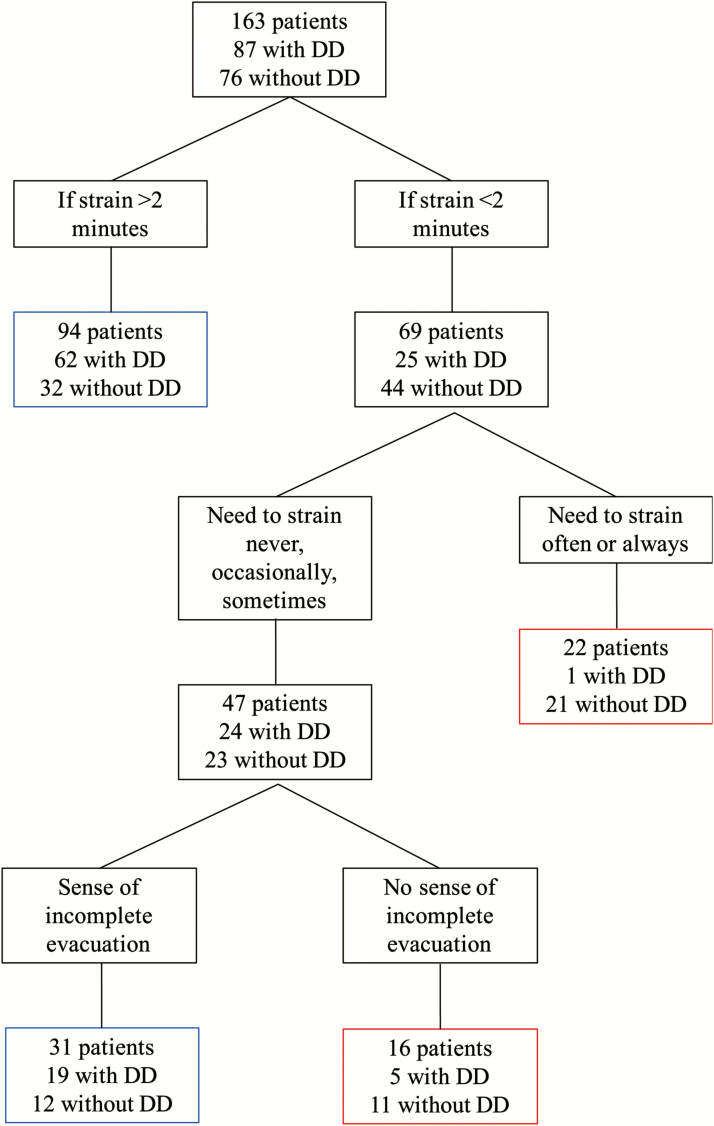
In this study, 166 consecutive English-speaking patients with CC who were referred for ARM completed a symptom questionnaire. DD was diagnosed if pelvic floor dyssynergy was demonstrated by ARM and balloon expulsion time was more than one minute. Likelihood ratios (LRs) were calculated for individual symptoms and prespecified symptom combinations. Likelihood ratios greater than five or less than 0.2 were considered significant. A recursive partitioning tree was used to find the symptoms best able to predict DD.
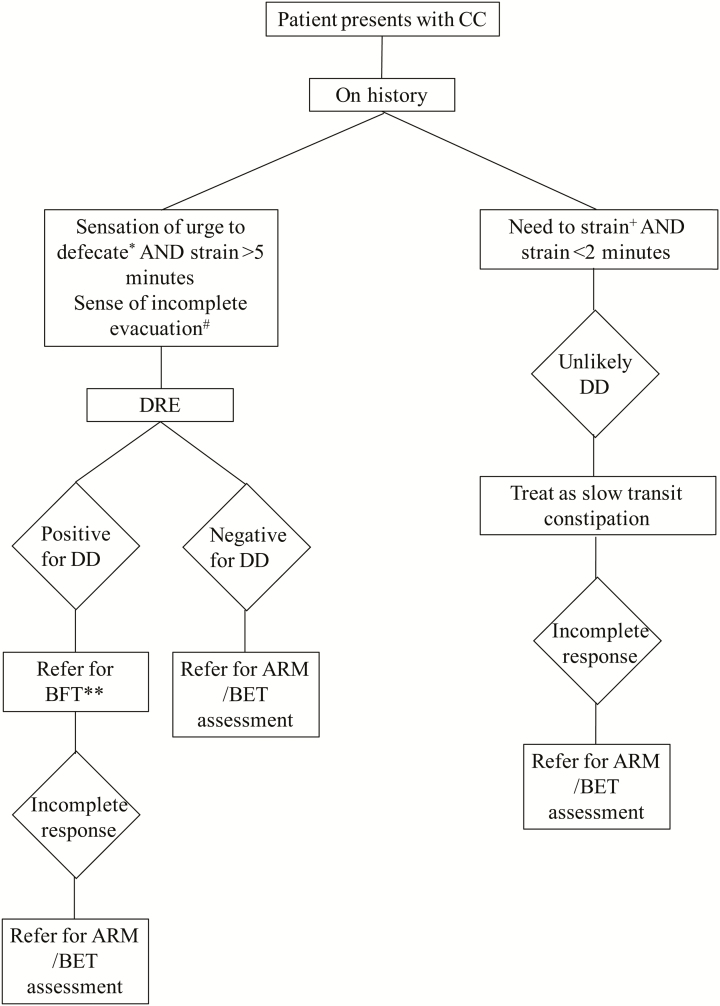
No single constipation symptom was sufficient to predict a diagnosis of DD. Patients who reported sometimes feeling an urge to defecate and a prolonged straining duration of greater than five minutes were more likely to have DD (LR = 7.74). In patients who reported straining often or always and had a short straining duration of less than two minutes, the diagnosis of DD was less likely (LR = 0.04). The recursive partitioning tree analysis similarly identified a sense of urge with a prolonged straining duration as predictor for DD, as well as an incomplete evacuation as another potential predictor.
Questions regarding need to strain, duration of straining, urge to defecate, and incomplete evacuation are useful to predict the presence of DD in patients with CC. These questions will enable clinicians to make a clinical diagnosis of DD to guide treatment.
排便协同失调(DD)存在于约30%的特发性慢性便秘(CC)患者中。DD的诊断标准需要客观测试,如肛门直肠测压(ARM);然而,在加拿大,ARM仍然是一种有限的资源。本研究的目的是使用标准化的自我报告症状问卷来确定CC患者中DD的可预测性。
在本研究中,166名连续转诊接受ARM检查的英语为母语的CC患者完成了症状问卷。如果ARM显示盆底协同失调且球囊排出时间超过1分钟,则诊断为DD。计算了个体症状和预先指定的症状组合的似然比(LRs)。似然比大于5或小于0.2被认为具有显著性。使用递归划分树来寻找最能预测DD的症状。
没有单一的便秘症状足以预测DD的诊断。报告有时有排便冲动且用力排便持续时间超过5分钟的患者更有可能患有DD(LR = 7.74)。在报告经常或总是用力排便且用力排便持续时间短于2分钟的患者中,DD的诊断可能性较小(LR = 0.04)。递归划分树分析同样确定,有排便冲动且用力排便持续时间延长是DD的预测指标,以及排便不尽是另一个潜在的预测指标。
关于用力排便的需要、用力排便的持续时间、排便冲动和排便不尽的问题有助于预测CC患者中DD的存在。这些问题将使临床医生能够对DD做出临床诊断以指导治疗。