Section of Nephrology, University of Chicago, Chicago, IL.
Division of Nephrology, Tufts Medical Center.
Am J Kidney Dis. 2019 Nov;74(5):620-628. doi: 10.1053/j.ajkd.2019.05.014. Epub 2019 Jul 10.
RATIONALE & OBJECTIVE: Identifying patients who are likely to transfer from peritoneal dialysis (PD) to hemodialysis (HD) before transition could improve their subsequent care. This study developed a prediction tool for transition from PD to HD.
Retrospective cohort study.
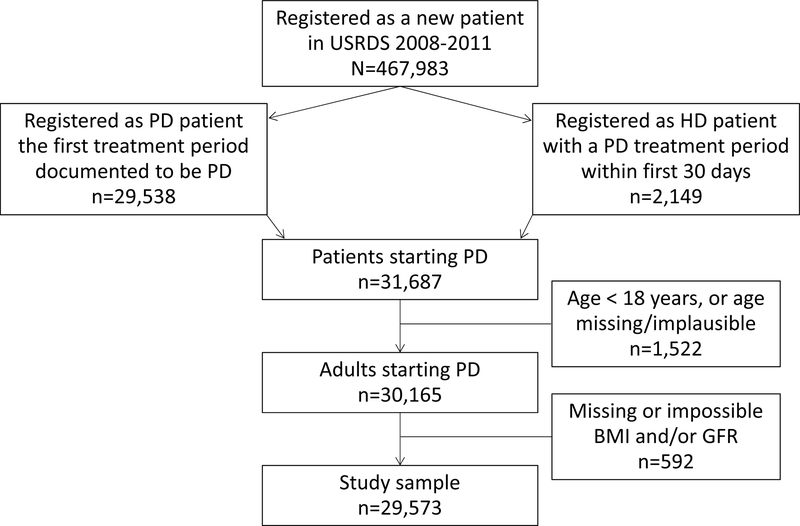
SETTING & PARTICIPANTS: Adults initiating PD between January 2008 and December 2011, followed up through June 2015, for whom data were available in the US Renal Data System (USRDS).
Clinical characteristics at PD initiation and peritonitis claims.
Transfer to HD, with the competing outcomes of death and kidney transplantation.
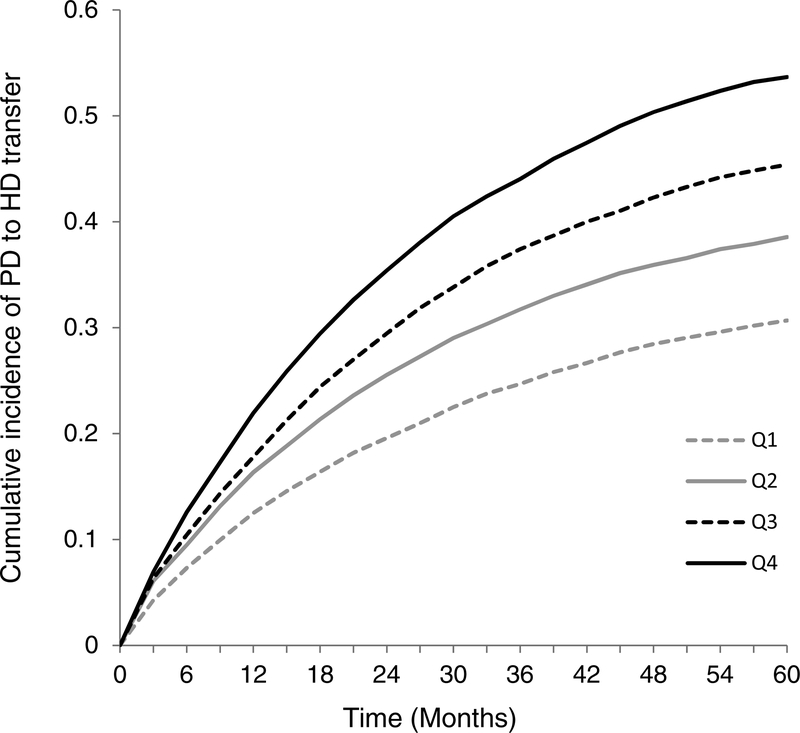
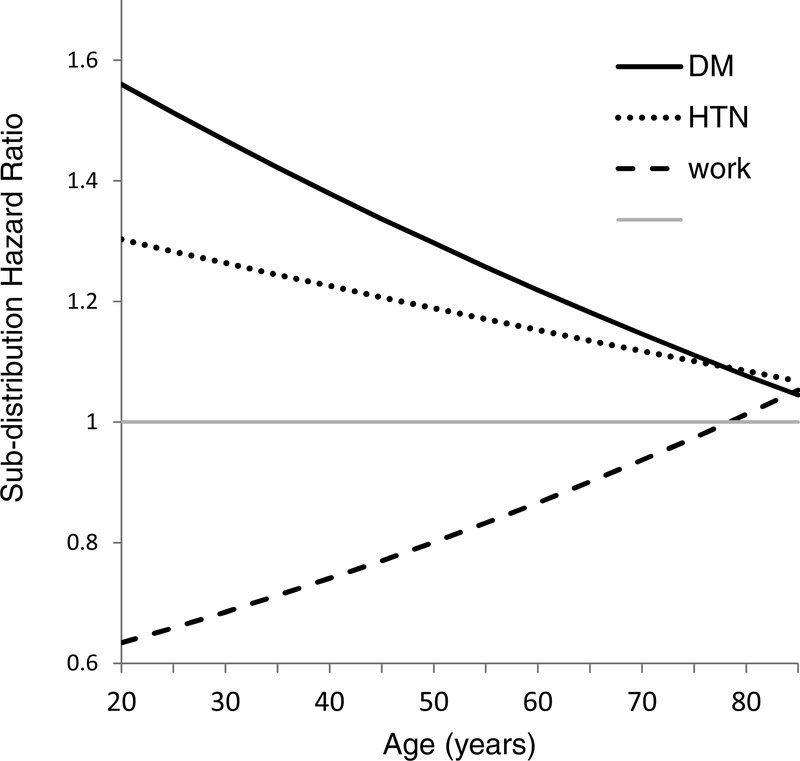
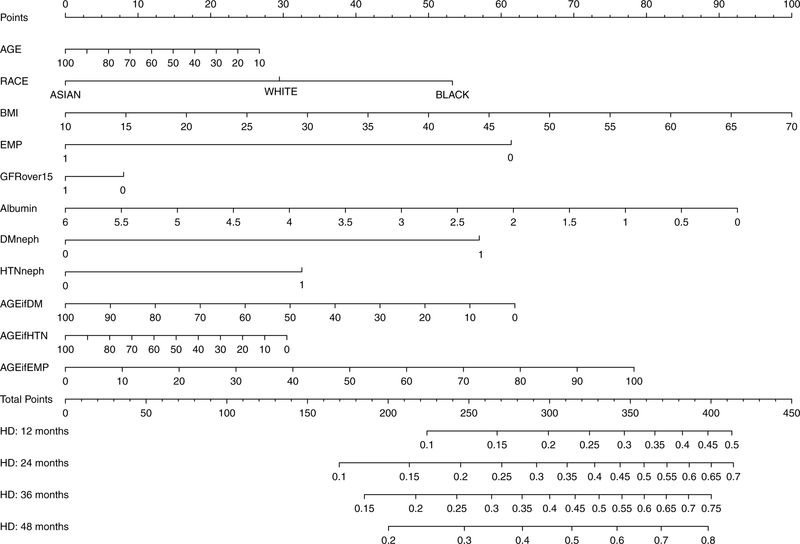
Outcomes were ascertained from USRDS treatment history files. Subdistribution hazards (competing-risk) models were fit using clinical characteristics at PD initiation. A nomogram was developed to classify patient risk at 1, 2, 3, and 4 years. These data were used to generate quartiles of HD transfer risk; this quartile score was incorporated into a cause-specific hazards model that additionally included a time-dependent variable for peritonitis.
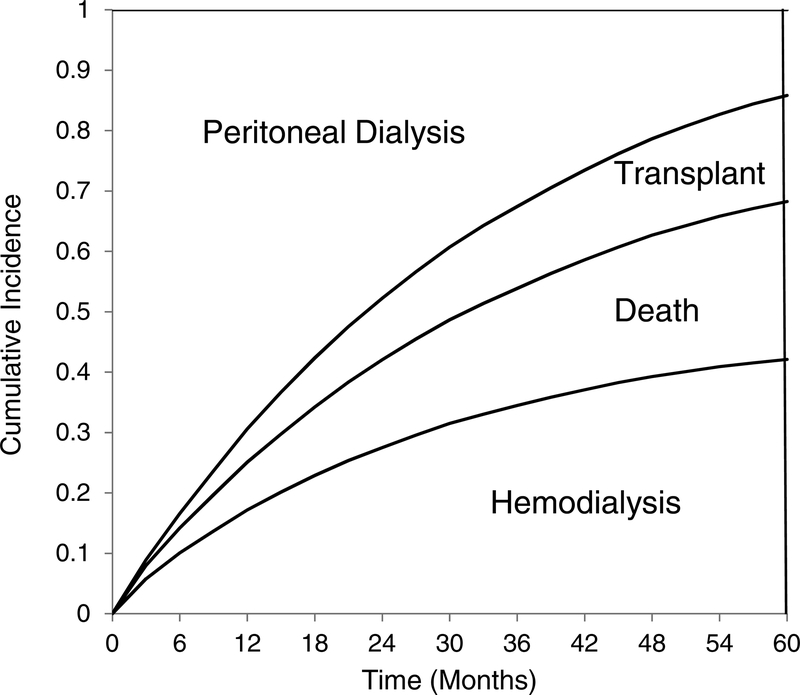
29,573 incident PD patients were followed up for a median of 21.6 (interquartile range, 9.0-42.3) months, during which 41.2% transferred to HD, 25.9% died, 17.1% underwent kidney transplantation, and the rest were followed up to the study end in June 2015. Claims for peritonitis were present in 11,733 (40.2%) patients. The proportion of patients still receiving PD decreased to <50% at 22.6 months and 14.2% at 5 years. Peritonitis was associated with a higher rate of HD transfer (HR, 1.82; 95% CI, 1.76-1.89; P < 0.001), as were higher quartile scores of HD transfer risk (HRs of 1.31 [95% CI, 1.25-1.37), 1.51 [95% CI, 1.45-1.58], and 1.78 [95% CI, 1.71-1.86] for quartiles 2, 3, and 4 compared to quartile 1 [P < 0.001 for all]).
Observational data, reliant on the Medical Evidence Report and Medicare claims.
A large majority of the patients who initiated renal replacement therapy with PD discontinued this modality within 5 years. Transfer to HD was the most common outcome. Patient characteristics and comorbid diseases influenced the probability of HD transfer, death, and transplantation, as did episodes of peritonitis.
在进行转换之前,识别可能从腹膜透析(PD)转为血液透析(HD)的患者,可改善其后续治疗效果。本研究旨在开发一种 PD 转 HD 的预测工具。
回顾性队列研究。
2008 年 1 月至 2011 年 12 月期间开始 PD 治疗、并随访至 2015 年 6 月的成年人,其数据可在美国肾脏数据系统(USRDS)中获得。
PD 起始时的临床特征和腹膜炎索赔。
HD 转归,以死亡和肾移植为竞争结局。
结局从 USRDS 治疗史文件中确定。使用 PD 起始时的临床特征拟合亚分布风险(竞争风险)模型。开发了一个列线图来对 1、2、3 和 4 年的患者风险进行分类。根据 HD 转归风险的四分位数对这些数据进行分组;该四分位评分被纳入一个包含腹膜炎时间依赖性变量的特定原因风险模型中。
共纳入 29573 例新发生的 PD 患者,中位随访时间为 21.6(四分位距 9.0-42.3)个月,其中 41.2%的患者转为 HD,25.9%的患者死亡,17.1%的患者接受了肾移植,其余患者随访至 2015 年 6 月研究结束。11733 例(40.2%)患者有腹膜炎索赔。PD 治疗的患者比例在 22.6 个月时降至<50%,5 年后降至 14.2%。腹膜炎与 HD 转归率较高相关(HR,1.82;95%CI,1.76-1.89;P<0.001),HD 转归风险四分位数评分较高也与 HD 转归率较高相关(四分位 2、3 和 4 组的 HR 分别为 1.31[95%CI,1.25-1.37]、1.51[95%CI,1.45-1.58]和 1.78[95%CI,1.71-1.86],与四分位 1 组相比,P<0.001)。
观察性数据,依赖于医疗证据报告和医疗保险索赔。
大多数开始接受 PD 肾脏替代治疗的患者在 5 年内停止了该治疗方式。HD 转归是最常见的结局。患者特征和合并症影响 HD 转归、死亡和移植的概率,腹膜炎发作也有影响。